

Albumin for sepsis resuscitation in the ED (ICARUS-ED)
What if albumin were given earlier in the course of sepsis?


Albumin hasn’t been consistently shown to be beneficial in the management of sepsis with hypotension or hypoperfusion when given in the ICU:

But this phase of care often begins hours after initial resuscitation efforts for sepsis have begun in the emergency department.
Could earlier administration of albumin in the ED be beneficial?
ICARUS-ED
What They Did
At a single center in Australia, 464 patients with “sepsis”—suspected infection plus suspected hypoperfusion due to systolic blood pressure <90 mm Hg or lactate >4 mmol/L—were randomized 1:1 to receive either open-label albumin (400 mL of 20% albumin infused over 4 hours) or usual care (i.e., crystalloids for resuscitation).
Almost all patients (95%) had a final clinical diagnosis of sepsis (presumed or confirmed infection) based on discharge summaries.
The primary outcome was systolic blood pressure at 24 hours, with numerous prespecified secondary outcomes. This was a pilot study, not adequately powered to test a mortality benefit.
What They Found
There was no difference in SBP at 24 hours (110.5 vs 110.0 mm Hg).
Patients receiving albumin had a statistically significant but small increase in their SBP at 6 hours: 108 vs 102 mm Hg.
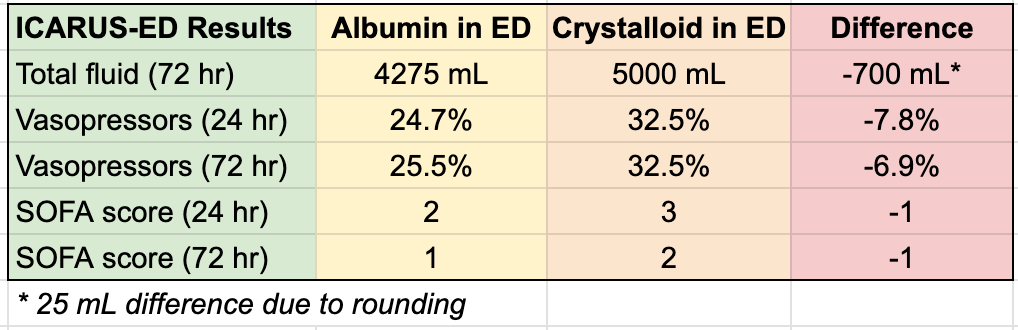
They received less total fluid volumes (by -700 mL at 24 hours), required vasopressors less often (-8%), and had lower organ failure scores (-1 point):
The trial was not powered to detect a mortality difference. Albumin-treated patients had an absolute 5% lower mortality in-hospital (28% vs 33%), not statistically significant, and a 2% increased mortality at 30 days (also not significant).
What It Means
ICARUS-ED echoes the findings of many other trials testing albumin in sepsis: fewer fluids infused, reduced vasopressor use, and lower organ failure scores, suggesting the agent is benefiting patients in some way.
However, albumin has had no clear effect on hard outcomes like mortality. ICARUS-ED does not inform this question meaningfully, as it was not powered to detect mortality differences.
Many people likely concluded from the rock-solidly negative SAFE trial (NEJM 2004) that there can be no conceivable mortality benefit from albumin. However, SAFE used 4% albumin, in contrast to the 20-25% preparations in wider use.
Numerous trials and meta-analyses testing concentrated albumin in sepsis tend to show physiologic improvements, and even a potential mortality benefit. ICARUS-ED’s dataset will soon be incorporated into updated meta-analyses to further inform the question.
Even if a benefit were found, there are major practical obstacles to expanded use of albumin. On a population basis, albumin is prohibitively expensive as a resuscitation fluid, costing hundreds or thousands of dollars per patient, compared to ~$10 for a similar treatment course with crystalloids.
Nor could the current production system accommodate the massive increase in scale that widespread use of albumin in ICUs would require.
But for those to become relevant concerns, albumin would first need to be demonstrated to show a clear mortality benefit in sepsis or another disease process.
After 40 years in this profession, I find it amusing how we keep trying to prove that albumin is of use for almost any condition, outside of specific circumstances involving cirrhotic patients. "It just makes SO much sense. It HAS to work." For my entire career people have been trying to prove that it works, and I do mean that it was an argument even when I was a medical student and before I actually had a career. There must be big profits in it; what other drug do you know that has failed over and over to show efficacy but is still marketed? For heaven's sake, drotrecogin alpha at least had one study that demonstrated a survival benefit, and it doesn't even exist any more. I love how the nephrologists persist in believing that albumin helps with dialysis and/or diuresis. Which it might do, but in our critical care patients all it evidently does is prolong the inevitable at great expense. The notion is so tempting that "we" keep doing trial after trial. The outcomes of the ICARUS-ED trial are non-sequiturs; unless they translate to a survival benefit, they mean nothing. I suppose I understand publishing the data, from an academic standpoint. It does seem fair that unless you can show these intermediate outcomes, you clearly will not be able to show a mortality outcome. If it spurs another multimillion dollar, multi-center RCT, perhaps it has some utility. At least we will be just about out of permutations on the theme. If it works, great. If it doesn't, I'm not sure where else we'll turn in the quest to prove that IT REALLY DOES WORK! The sirens keep calling...
If they use less vasopressors and have less organ failure, isn't this success? Why do we always use mortality as an endpoint? If the ones who end up surviving do so with less damage, isn't this a good thing?