

An Expected or Maladaptive Response to Infection? Sepsis Reconsidered

Jon-Emile S. Kenny [@heart_lung]
“A man may take to drink because he feels himself to be a failure, and then fail all the more completely because he drinks … English … becomes ugly and inaccurate because our thoughts are foolish, but the slovenliness of our language makes it easier for us to have foolish thoughts.”
George Orwell reminds us to be accurate and clear in our language, and this may be at the center of the current upheaval surrounding the Third International Consensus Definitions for Sepsis and Septic Shock. There is already great debate pertaining to the use of the SOFA score or the qSOFA score, rather than SIRS criteria to define sepsis. What is most important – to my eye, at least – is the new verbiage. The term ‘sepsis’ is a human-borne construct, it does not objectively exist in the world as does a pneumococcal pathogen or a molecule of cefepime. ‘Sepsis’ may be defined however we see fit. Previously, sepsis meant a presumed infectious source plus at least two systemic inflammatory response syndrome [SIRS] criteria. Now, sepsis has been redefined as a life-threatening organ dysfunction caused by a dysregulated response to infection. The debate as to whether or not this is appropriate will wage for a while, but I can appreciate the intention of the authors. In their new definition, sepsis is a clinical state which is considered excessive, maladaptive and abnormal. This is in contradistinction to the old paradigm whereby the systemic inflammatory response syndrome is considered to be a ubiquitous and perhaps, adaptive host response – does a commonplace host response to infection warrant the term ‘sepsis?’ The current authors clearly think not.
While the old and new definitions of ‘sepsis’ are different, I do not believe that the clinician’s approach to the infected patient will change any more than the management of infected patients will change in response to the ARISE, ProCESS and ProMISe trials. We will still ultimately ask ourselves the same three fundamental questions: 1. Is the patient infected? 2. Is there life-threatening end-organ dysfunction? 3. Is there shock? [figure 1].
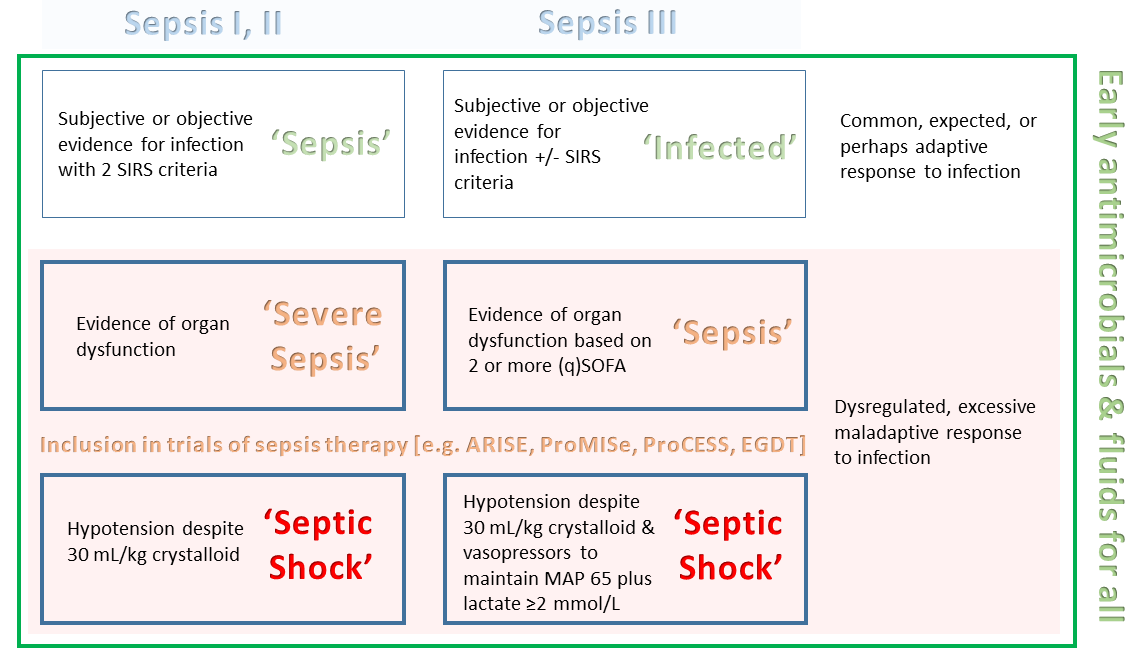
Is the patient infected?
Neither the old nor the current definitions of sepsis can answer this question. The question of infection is a clinical gestalt and varies from one infectious disease to another. A presumed source of pneumonia conjures up very different diagnostic criteria than an infected biliary tree or heart valve. While each infection may have multiple diagnostic criteria with varying sensitivity and specificity, many inherently include the SIRS criteria [especially fever and leukocytosis]. Consider a patient with fever, leukocytosis, and a Murphy’s sign – throw in jaundice and you’ve met Charcot’s Triad. Is this patient infected? Almost certainly. Does this patient have life-threatening organ dysfunction caused by a dysregulated response to infection? If not – by the current definition – this patient is infected, but not septic. Does this modification in diagnostic classification change therapeutics? No. Importantly, in the new definition, SIRS is not abandoned; the authors are very clear that the SIRS criteria are still a valuable utensil for the diagnosis of ‘infection.’ The authors argue, however, that meeting at least 2 SIRS criteria does not accurately identify patients with life-threatening organ dysfunction, at least as compared to the SOFA score.
Is there life-threatening end-organ dysfunction?
The implicit use of SIRS criteria to aid in the diagnosis of infection [above] is so strong, that their elimination from the current taxonomy impels us towards the qSOFA and SOFA as surrogates for the diagnosis of infection. The most important point here is that the use of the qSOFA and SOFA scores cannot be used to diagnose infection; indeed, they were derived in patients with a high pre-test probability of having infection [presumably based on clinical gestalt described above]; their utility, therefore, is in predicting mortality – i.e. life-threatening end-organ dysfunction. Debating the sensitivity and specificity of these scores to diagnose infection is moot; that is not how they were derived nor was it the intention of the authors. It would be somewhat akin to debating the use of troponin and BNP in the diagnosis of pulmonary embolus. Thus, the use of qSOFA and SOFA do not replace SIRS in the diagnosis of infection as described above. qSOFA and SOFA are an – albeit imperfect – attempt to augment the predictive power of organ dysfunction and mortality.
By the old definition, the presence of organ dysfunction heralded ‘severe sepsis’ which has been deemed redundant by the use of the SOFA criteria. Accordingly, the new term ‘sepsis’ is strikingly similar to the old term ‘severe sepsis.’ The key difference between the old and the new is that 'severe sepsis' included any one organ dysfunction, while the new definition essentially requires two. Consider the patient above with an infected biliary tree. If that patient develops altered sensorium with hypotension – he has met Reynold’s Pentad – and now has a maladaptive, excessive and life-threatening organ dysfunction in response to infection. Previously, this patient would be diagnosed as having at least ‘severe sepsis’ and would have met inclusion criteria in any of the major trials of sepsis therapy [e.g. ProMISe, ProCESS, ARISE, EGDT]. By the new definition, this patient is ‘merely’ septic but a simple change in terminology – I pray – will not delay the patient in being evaluated for admission to the ICU and a modern approach to early goal directed therapy [EGDT].
Is there shock?
The current definition does also depart somewhat from the older definition of shock. Previously, shock demanded persistent hypotension in the face of adequate volume resuscitation – 30 mL/kg of crystalloid. Now, in the face of adequate volume replacement, vasopressors to maintain a mean arterial pressure of at least 65 mmHg and the presence of an elevated lactate are essential. The reason for this change was, as above, based on empiric evidence. Once again, this new definition should not alter management.
Final thoughts
It is a fair criticism that under-treatment is risked by essentially requiring two organ systems to fail within the new paradigm and I wholeheartedly appreciate the concerns raised with respect to a ‘new’ definition of sepsis; however, this heightened fear is reminiscent of the trepidations raised by clinicians clinging to the classic EGDT protocol in the aftermath of the ProCESS, ProMISe and ARISE trials. While I am no strong proponent of this revised classification, I find it hard to accept the perception that clinicians everywhere will quickly and embarrassingly lose their bearings when diagnosing and managing life-threatening infection; we are too smart for that. I remain confident that all infected patients – with or without organ dysfunction and shock – will continue to receive prompt, aggressive care regardless of how we label them.
Humbly [from he who defends the central venous pressure],