

Balanced solutions: better than saline, but which balanced solution?
Vandy tests Normosol-R vs. Lactated Ringers

Balanced crystalloids are considered to be probably superior to normal saline as a resuscitation fluid in critically ill patients. But there are multiple balanced crystalloid products available, with varying compositions.
Does the choice of balanced solution make a difference in patient outcomes from critical illness?
Balanced solutions are formulated with electrolyte and solute concentrations closer to plasma’s, compared to normal saline’s simple composition of sodium and chloride (154 mEq/L each).
Large randomized trials and meta-analyses suggest that using balanced crystalloids instead of normal saline might (very slightly) reduce acute kidney injury and mortality in critically ill patients. With more than 20 million patients treated in ICUs annually worldwide, even a small postulated effect size (e.g., ~1%) could be significant.
More on balanced solutions from PulmCCM:


Acid-Base Oversimplification 101
How are buffered solutions better than saline, or at least more balanced? Normal saline has an equal number of cations (sodium of 154 mEq/L) and anions (chloride at 154 mEq/L), and no buffers. It has a “strong ion difference” of zero.
When infused into the bloodstream, the relative excess of chloride ions can reduce bicarbonate in the blood, producing a hyperchloremic metabolic acidosis.
This acidosis is postulated to cause or worsen renal failure (SMART trial, SALT-ED trial) and possibly mortality (meta-analyses).
Buffered solutions do not acidify the blood, and instead alkalinize it slightly. Their buffering ions—lactate, acetate, or gluconate—act as precursors to bicarbonate, and create a strong ion difference of 24-50 mEq/L.
Types of Balanced Crystalloids
There are two major types of balanced crystalloids:
Microelectrolyte solutions buffered with gluconate, acetate, or both (Normosol-R and Plasmalyte-A are two major brands);
Lactated Ringers and Hartmann’s solution contain lactate as their buffer.
Here’s how the solutions vary:
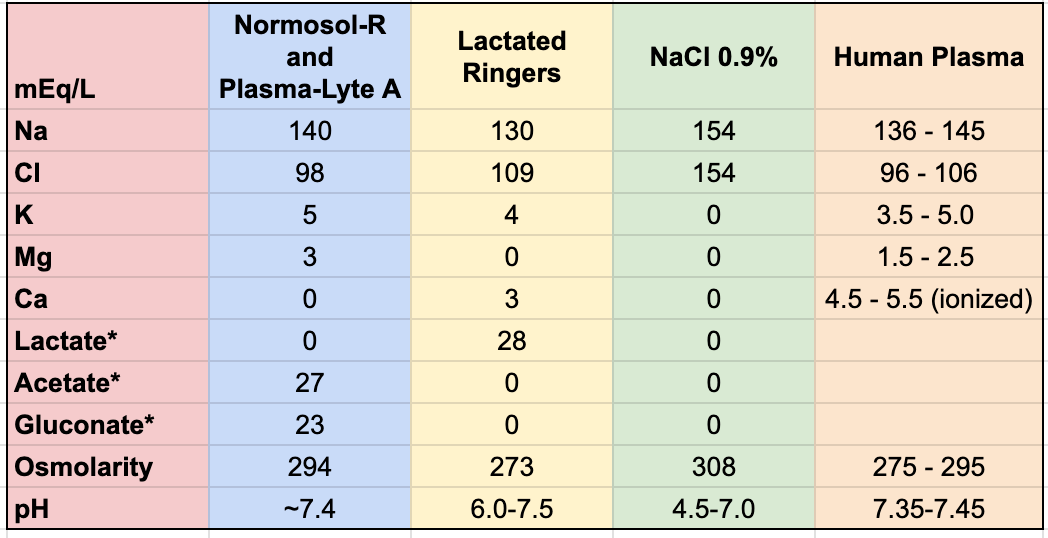
There are only minor differences in composition between the two categories of balanced crystalloids (blue and yellow columns in the chart).
Buffering capacity (i.e., strong ion difference) is also quite similar for LR (28 mEq/L) and Normosol-R (24 mEq/L), while Plasma-Lyte A’s is significantly higher (50 mEq/L). The strong ion difference of plasma is about 40 mEq/L.
Based on their similarities, you might expect no differences in outcomes between patients resuscitated with LR or Normosol-R.
But researchers at Vanderbilt, where the SMART study testing balanced crystalloids was performed, checked—just to be sure.
Normosol-R versus Lactated Ringers in the Critically Ill: RCT
In a pragmatic, cluster-randomized, multiple-crossover trial, investigators randomized 2,084 patients at a single ICU at Vanderbilt to receive either Normosol-R or LR as their resuscitation fluid, between 2018 and 2019.
They essentially kept flipping the unit en bloc back and forth monthly between using one fluid or the other, then observed, combined and compared outcomes from the various epochs according to which fluid had been in use. The study was unblinded.
The primary outcome was plasma bicarbonate concentration between enrollment and 7 days, with secondary outcomes of need for renal replacement therapy, 30-day mortality, acid-base status, organ failure, etc.
There were no significant differences in any outcome:
Bicarbonate levels: (-1.2 mmol/L, lower in Normosol)
Dialysis/CRRT: (6% Normosol vs 5% LR, 95% CI, -1.2% to 3.1% for the difference)
Mortality (16.3% Normosol vs 16.0% LR)
No significant differences in plasma sodium, chloride, potassium, pH, or base excess or strong ion differences.
What to make of the numeric increase in the need for RRT among patients receiving Normosol? Probably nothing, and a much larger trial (n~16,000) would be needed to identify a 1% difference at that low incidence.
Conclusions
This was a relatively low-stakes and small-scale effort to look for differences in bicarbonate concentration between balanced solutions infused—which, even if positive, would have been a far-extrapolated distance from clinical significance.
As a comparison, the SMART trial (NEJM 2018), performed at five ICUs at Vandy, enrolled 16,000 subjects to find meaningful clinical differences between balanced solutions and normal saline.
As this trial showed no danger signs with the use of LR, it’s a “positive” trial for healthcare costs. Lactated Ringer’s costs about $2 less per liter than Normosol-R, which in turn is about $2 cheaper per liter than Plasma-Lyte.
This is great. Never even heard of Normosol-R, and we likely won't be able to get it. I use LR almost exclusively on my patients (unless they are very hyperkalemic) and then use Plasmalyte for my liver failure patients, so the lactate doesn't accumulate.