

How long should CPR be performed for non-shockable cardiac arrests in the hospital?
A series to help inform the final life-and-death decision


This is part of a series of articles on the duration of CPR for in-hospital cardiac arrest. An index to all posts in the series can be found here:

Introduction
Although cardiopulmonary resuscitation (CPR) is performed on more than 250,000 people in U.S. hospitals each year, physicians receive no formal guidance or training on how long it should be performed.
This results in a wide variation in practice—25% of unsuccessful resuscitations are stopped before 15 minutes, while an equal number go longer than 30 minutes. The other half range between 15 and 30 minutes, with a median of about 21 minutes.

This series of posts reviews the data that can support clinicians in making the ultimate life-and-death decision: stopping CPR in the hospital.
Here we examine the most common category of cardiac arrests, which also have the worst outcomes: nonshockable rhythms. But first, a quick recap of what we know about all in-hospital cardiac arrests and shockable cardiac arrests.
“Lumping” All In-Hospital Cardiac Arrests Loses Important Nuance
Overall, about two-thirds of patients survive their initial in-hospital cardiac arrest, but two-thirds of them subsequently die in the hospital. About one-quarter of all in-hospital arrest patients survive to hospital discharge.
Most (historically 60-75%, more recently up to 85%) of those who survive their arrest to be discharged from the hospital have good functional status (mild-to-moderate disability or none, able to function independently). That’s about 15-20% of all inpatient cardiac arrests.
Both survival to hospital discharge and survival with good functional status decline with a longer duration of CPR in a nonlinear fashion:
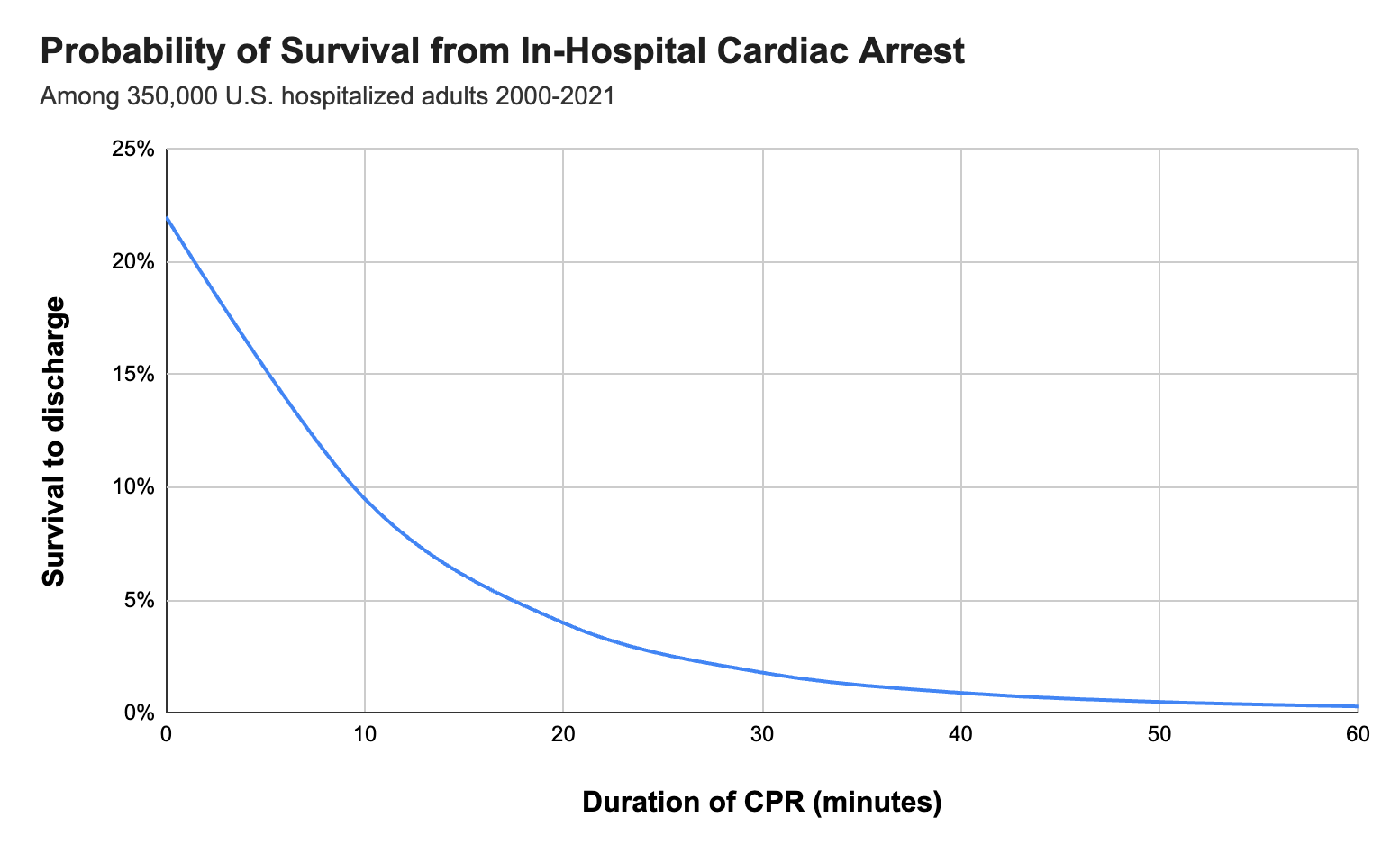
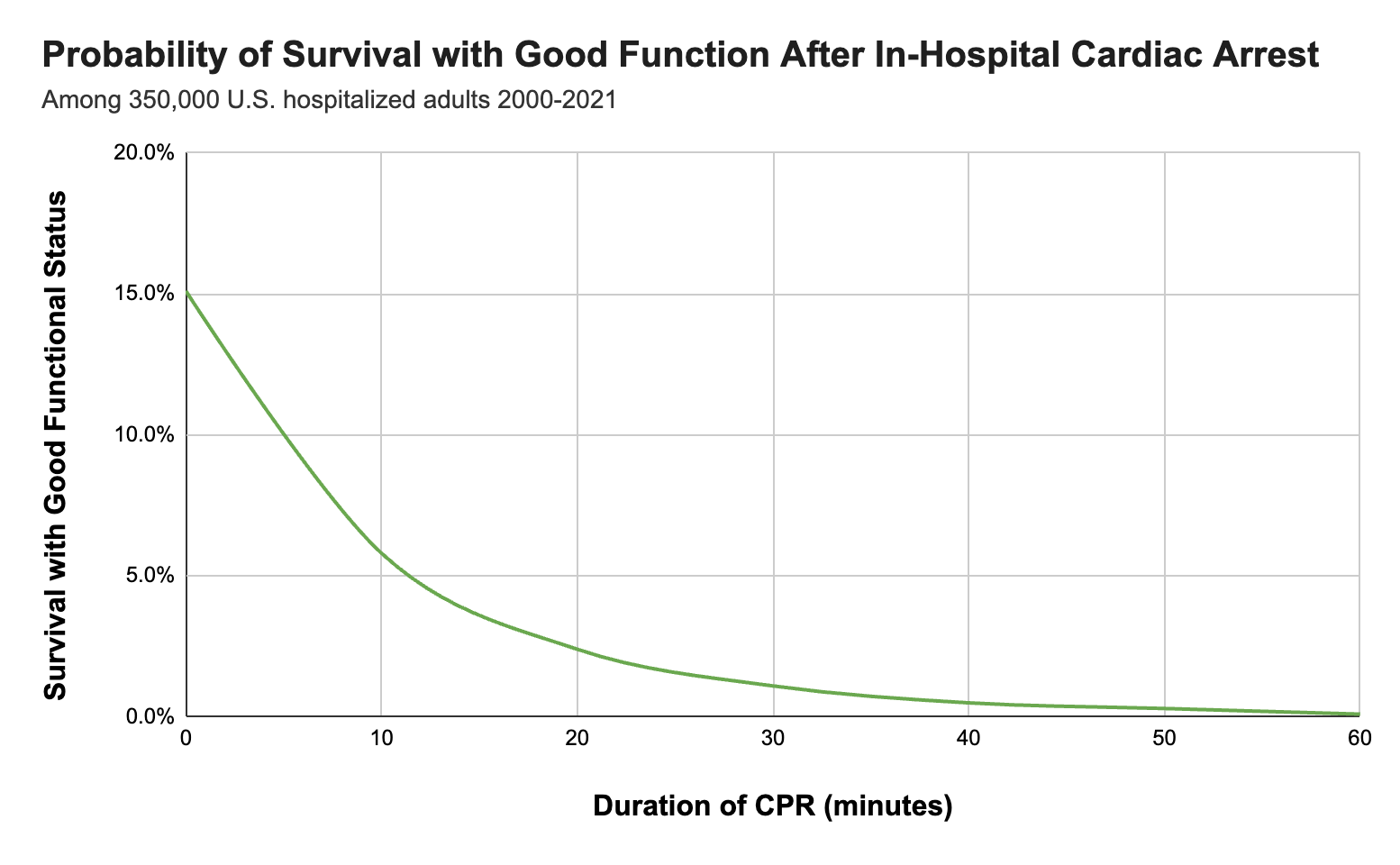
(If you’re reading this in an email, click the post title for a better view of the plots on the website or app.)
But as we saw in the last post, these plots lumping together all in-hospital arrests conceal important variability in the arrest types and in the patients themselves. This variation contributes to a wide spectrum in outcomes.
The most important distinction is of rhythm type.
Rhythm Type: Non-shockable vs Shockable
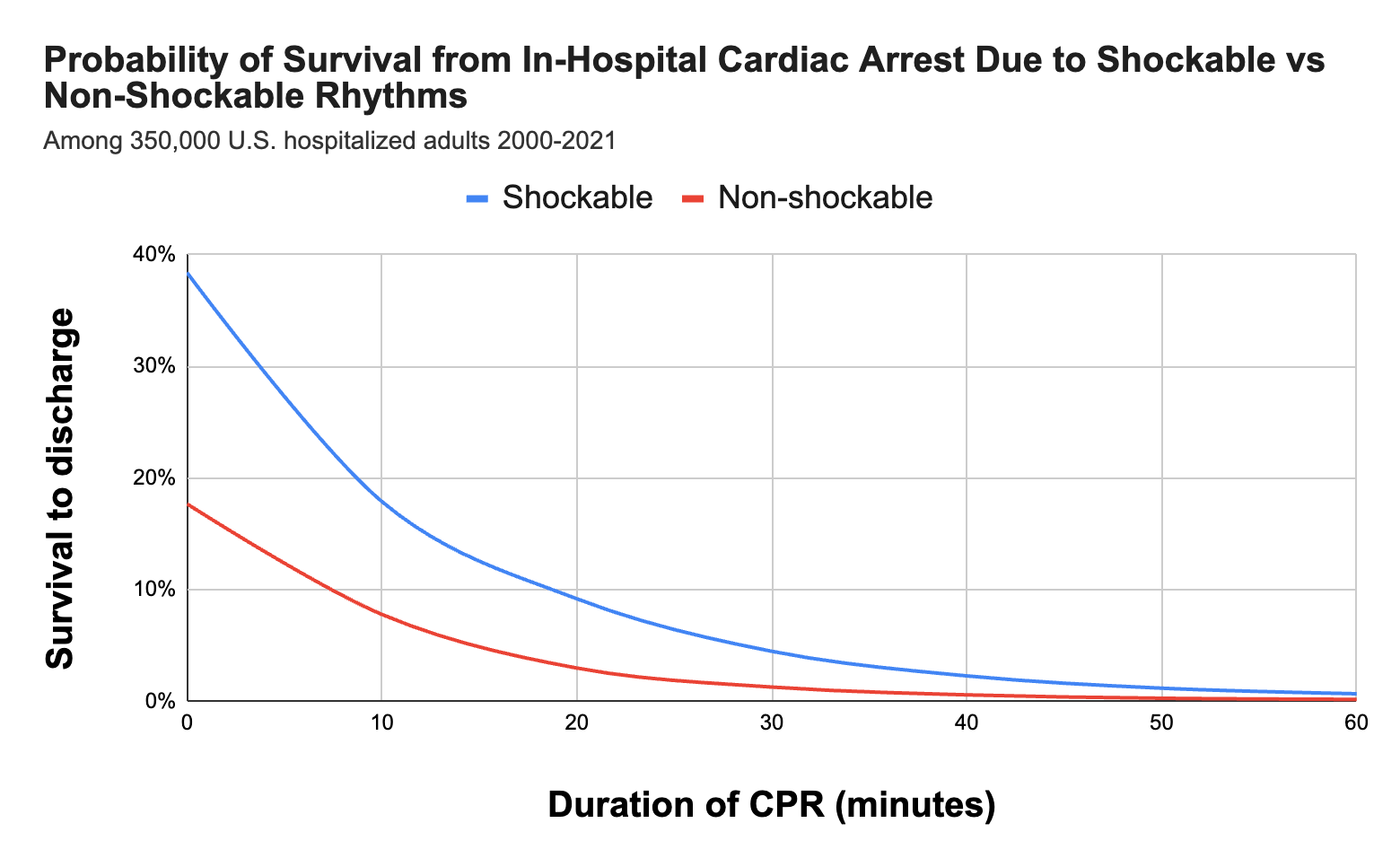
Patients with in-hospital cardiac arrests due to ventricular fibrillation (VF) and ventricular tachycardia (VT)—so-called shockable rhythms—receive different treatments (defibrillation and anti-arrhythmic drugs) and have better outcomes generally than those with non-shockable rhythms (asystole and pulseless electrical activity or PEA).
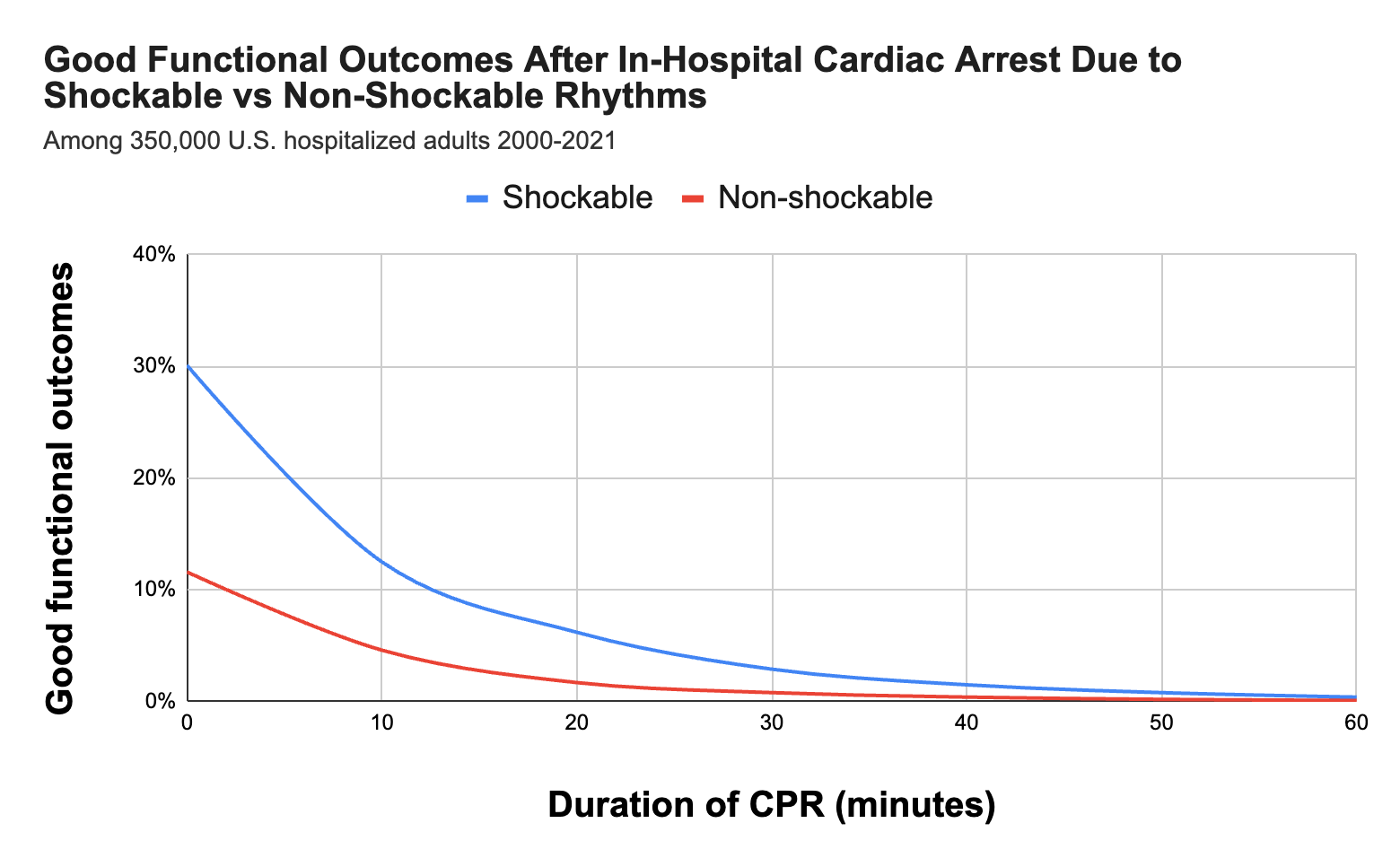
Although shockable rhythms are a minority of in-hospital arrests (~20%), roughly 40% survive to discharge, compared to only about 15% of patients with arrests due to non-shockable rhythms. A higher proportion of shockable arrest survivors also retain good function: as many as 30-40% leave the hospital neurologically intact.
As the duration of CPR increases from any arrest type, the likelihood of survival or freedom from neurologic disability both decrease.
And in table form:


Non-Shockable Arrest Management
A refresher for the usual management of in-hospital cardiac arrests due to PEA or asystole (refer to relevant publications for more detailed management advice):
Start CPR, pushing at least 2 cm in depth at 100-120 compressions per minute, delivering 2 breaths every 30 compressions unless an advanced airway is in place
Give epinephrine 1 mg every 3 to 5 minutes as soon as possible and consider an advanced airway and capnography
CPR for 2 minutes
Consider and address reversible causes/contributors: hypovolemia, hypoxemia, acidosis, hyper/hypokalemia, hypothermia, tension pneumothorax, cardiac tamponade, toxins, myocardial infarction, and pulmonary embolism. These “Hs and Ts” are most commonly associated with PEA/asystole arrests but should be considered in all cardiac arrests.
Repeat the cycle until ROSC is obtained, or until …. what, or when, exactly?
How Long To Keep Going?
Keep reading with a 7-day free trial
Subscribe to PulmCCM to keep reading this post and get 7 days of free access to the full post archives.