

ICU Physiology in 1000 Words: Venous Doppler & Volume Tolerance

Jon-Emile S. Kenny MD [@heart_lung]
With the birth of 'fluid responsiveness' physiology [1], there has been a slow and solemn drumbeat ushering the central venous pressure [CVP] up the squeaking planks of the hemodynamic gallows [2, 3]. Despite this, a few years ago I made a humble defense of the central venous pressure. Importantly, I was not proposing the CVP as a marker of fluid responsiveness or volume status; instead, I aimed to remind the reader that the CVP remains germane to cardiovascular physiology! Dismissing the CVP as ‘useless’ is analogous to deeming ‘stroke volume’ or ‘renal perfusion pressure’ as forgettable – for neither variable definitively speaks about a given hemodynamic state.
It is now possible that the CVP will rise again, for example, in the context of venous Doppler velocimetry. The venous Doppler waveform is an ultrasonographic transduction of the CVP, right heart hemodynamics and, therefore, a potential non-invasive indicator of venous congestion and volume tolerance.
The Central Venous Pressure Waveform
Classically, teaching of the CVP [or right atrial pressure - Pra] waveform begins with the a-wave [see figure 1A] [4-7]. Note that, while the a-wave is the rise in Pra due to atrial contraction, it is the end of ventricular diastole. The key determinants of the height of the a-wave are atrial volume and compliance. Because the relationship between atrial volume and pressure is curvilinear [8, 9], higher atrial volume leads to increasingly great pressure. Thus, large a-waves typically indicate a large atrial volume. The cannon a-waves of atrioventricular dissociation – atrial contractions against a closed tricuspid valve – are often taught for examination purposes, but are rare clinically.
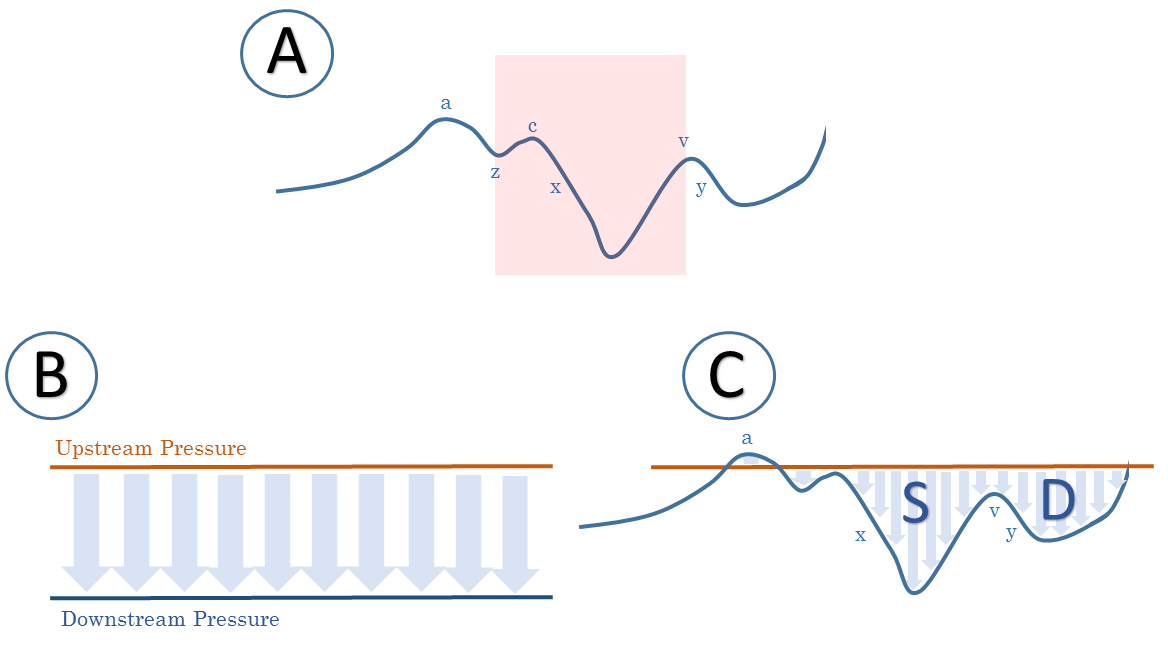
Figure 1: A - the CVP or Pra waveform tracing; see text for details, red-shade represents systole. B - generic depiction of flow detected by pulsed wave Doppler with static upstream [orange] and downstream [blue] pressures resulting in monophasic waveform. C - Pulse wave Doppler with variable downstream pressure [blue - right atrial pressure]. S is systolic wave towards heart, D is diastolic wave towards heart. This analysis assumes a constant upstream pressure [in orange]; it also assumes a constant vessel diameter as flow = [vessel area] x measured velocity.
As the atrium relaxes, the pressure falls towards the end-diastolic pressure [EDP]. This, z-point, is found at the base of the a-wave just prior to the – commonly indistinguishable – c-wave [4, 5, 10]. When systole begins, there is a moment when right ventricular [RV] pressure rises against closed tricuspid and pulmonic valves [i.e. isovolumic contraction]. Here, the tricuspid valve projects backwards into the right atrium resulting in a brief increase in pressure – the c-wave – until the pulmonic valve opens and ventricular blood ejects forward into the pulmonary tree; systole progresses [11].
During systole, the tricuspid annulus is pulled downwards towards the apex of the heart. This motion lowers the pressure in the right atrium – termed the x-descent [11]. It follows that this fall in right atrial pressure during systole is primarily determined by 1. Systolic function and 2. A competent tricuspid valve. Accordingly, if there is either poor ventricular function or a leaking tricuspid valve, the x-descent is partially or wholly erased.
As systole progresses, the tricuspid annulus shifts backwards towards the cardiac base while meeting on-going venous return within the right atrium; consequently, pressure rises – the v-wave. Like the a-wave, the height of the v-wave is primarily determined by atrial volume and compliance. Normally, the v-wave is not as high as the a-wave [4-6]. If, however, the atrium is volume overloaded, and/or poorly compliant, then the v-wave may be quite tall – potentially leading to a great y-descent, as described below.
When the tricuspid valve opens, diastole begins. The RV accepts volume from the atrium, so the Pra tumbles into the y-descent. Early diastolic ‘suction’ may facilitate the y-descent [6]; as well, the fall in pressure is particularly susceptible to respiratory variation – more so than the x-descent. This may be due to anatomical connection between the diaphragm and pericardium [12]. That is, with an inspiratory fall in the diaphragm, the capacitance of the pericardium and right ventricle increase and y-descent is enhanced. Normally, the RV is highly compliant; indeed, it acts as a ‘non-stressed’ chamber [13] such that following the y-descent there is little pressure change until atrial contraction at end-diastole.
Venous Doppler Velocimetry
What does the CVP or Pra tracing have to do with venous Doppler interrogation? When a clinician executes pulse wave Doppler analysis within a vein, there is an immediate up and down-stream pressure driving flow through the area of interest [see figure 1B]. But what if the down-stream pressure varies with time – as the Pra does? This is the genesis of the multi-phasic venous Doppler waveform [see figure 1C]. In other words, the CVP [i.e. Pra] tracing may be visually transduced at the bedside! This can be performed within the superior vena cava [SVC] [14], hepatic vein [HV] [15] and even the internal jugular vein [IJ] [16]. A similar physiology is also employed in the pulmonic vein to interrogate left atrial physiology [17].
Considering the SVC, it is well-established that the Doppler waveform behaves in a similar manner to the Pra tracing [14]. For example, in healthy individuals, inspiration increases both the x and y-descents, but the latter more so [14]. In the SVC tracing, there can be small amounts of ‘reverse’ flow which occur during atrial contraction and sometimes during the peak of the v-wave. In health, the degree of reverse flow is < 10% throughout the respiratory cycle [14] [see Figure 1C].
In the setting of pulmonary hypertension, tricuspid regurgitation and/or poor RV function, the venous Doppler profile follows the aberrations of the Pra tracing [18, 19]. With increased atrial volume, the a-wave enlarges thus augmenting reverse flow. Further, the systolic Doppler wave [i.e. x-descent] is progressively lost with poor RV function [19]; additionally, if the tricuspid valve is incompetent, then there may be reverse flow throughout all of systole [11] [see figure 2 B & C]! If atrial volume remains high at the end of systole, then the v-wave may lead to reverse flow and the diastolic Doppler wave [i.e. the y-descent] is prominent [19].
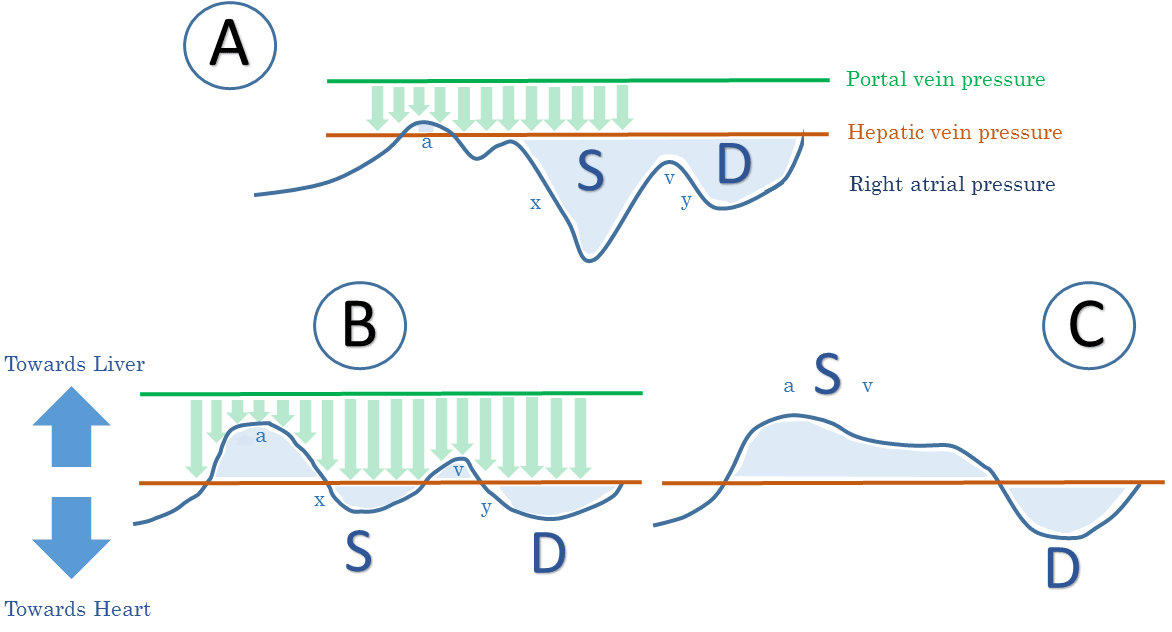
Figure 2: Schematic of portal vein [PV] pulsed wave Doppler interrogation [green - analysis between upstream PV pressure and hepatic vein [HV] pressure] and HV Doppler interrogation [blue - analysis between upstream HV pressure and downstream CVP] with progressively worsening tricuspid regurgitation [TR]. A is normal with minimal PV flow pulsatility [green flow profile]. B represents worsening disease with atrial congestion [tall a-wave] and diminished x-descent or S wave from systolic back-leak [i.e. TR]. PV pulsatility is enhanced because of atrial pressure reflection towards the PV. C represents severe TR with fused aSv wave; there is no x-descent because of severe back-leak during systole. Note that the fraction of flow towards the heart is diminished relative to back flow. This depicts worsening congestion of the abdominal organs.
Very similar physiology occurs in the hepatic veins [HV], however, in health there tends to be slightly more reverse flow than in the SVC [14]. Further, local pressure may alter the HV waveform considering that it is surrounded by the liver, within the abdominal cavity. Thus respiratory variation can render acquisition of the HV waveform more difficult [14]; especially with Valsalva, intra-abdominal hypertension or when collapse of the IVC ‘cuts-off’ the HV waveform from right atrial pressure variations [11].
Clinical Applications: volume tolerance includes volume responsiveness
Because the CVP marks the outlet pressure for venous return, capillary filtration and lymphatic drainage [6], its value is important for assessing organ congestion. Indeed, abnormal Pra tracings are reflected back into the portal vein. For example, portal vein flow normally undulates gently with a minimum at end-diastole and maximum during systole [see Figure 2 A & B]. This occurs because end-diastolic a-wave flow-reversal in the HV is reflected backwards into the liver, transiently shrinking the portal venous stream. Conversely, systole and early diastole ‘pull’ venous blood through the hepatic and, therefore, portal veins [11]. Accordingly, excessive portal pulsations suggest high venous retrograde flow – in other words, an RV under duress [see figure 2 B & C] [20]. Similar physiology has been observed within the intra-renal veins [21, 22].
In summary, right-heart venous Doppler provides an index of ‘volume tolerance’ for the abdominal organs just as pulmonary venous Doppler qualitatively assesses left atrial pressure and risk of pulmonary edema. These measurements, I believe, supplement the idea of ‘volume responsiveness’ which specifically refers to the heart’s ability to augment its stroke volume in response to preload. I think of ‘volume responsiveness’ as a sub-type of ‘cardiac volume tolerance;’ a heart on the flat portion of its Starling curve is volume intolerant. Conversely, a heart on the steep portion of its Starling curve may be feeding kidneys that are volume intolerant by venous Doppler. Thus, assessment of both arterial and venous sides of the circulation may provide nuance in fluid management.
Please check out other articles in this series,
For more information on the CVP tracing please check out chapter 6.
References
Michard, F. and J.L. Teboul, Using heart-lung interactions to assess fluid responsiveness during mechanical ventilation. Crit Care, 2000. 4(5): p. 282-9.
Marik, P.E., M. Baram, and B. Vahid, Does central venous pressure predict fluid responsiveness? A systematic review of the literature and the tale of seven mares. Chest, 2008. 134(1): p. 172-8.
Marik, P.E. and R. Cavallazzi, Does the central venous pressure predict fluid responsiveness? An updated meta-analysis and a plea for some common sense. Crit Care Med, 2013. 41(7): p. 1774-81.
Magder, S., How to use central venous pressure measurements. Current Opinion in Critical Care, 2005. 11(3): p. 264-270.
Magder, S., Central venous pressure: A useful but not so simple measurement. Crit Care Med, 2006. 34(8): p. 2224-7.
Magder, S., Central venous pressure monitoring. Current Opinion in Critical Care, 2006. 12(3): p. 219-27.
Magder, S., Right Atrial Pressure in the Critically Ill: How to Measure, What Is the Value, What Are the Limitations? Chest, 2017. 151(4): p. 908-916.
McNaughton, D.A. and M.M. Abu-Yousef, Doppler US of the liver made simple. Radiographics, 2011. 31(1): p. 161-188.
Khurram, I.M., et al., Association between left atrial stiffness index and atrial fibrillation recurrence in patients undergoing left atrial ablation. Circulation: Arrhythmia and Electrophysiology, 2016. 9(3): p. e003163.
Magder, S., Central venous pressure monitoring. Current opinion in critical care, 2006. 12(3): p. 219-227.
Scheinfeld, M.H., A. Bilali, and M. Koenigsberg, Understanding the spectral Doppler waveform of the hepatic veins in health and disease. Radiographics, 2009. 29(7): p. 2081-2098.
Magder, S., F. Erice, and D. Lagonidis, Determinants of the Y Descent and its Usefulness as a Predictor of Ventricular Filling. Journal of Intensive Care Medicine, 2000. 15(5): p. 262-269.
Pinsky, M.R., My paper 20 years later: Effect of positive end-expiratory pressure on right ventricular function in humans. Intensive Care Med, 2014. 40(7): p. 935-41.
Appleton, C.P., L.K. Hatle, and R.L. Popp, Superior vena cava and hepatic vein Doppler echocardiography in healthy adults. Journal of the American College of Cardiology, 1987. 10(5): p. 1032-1039.
Abu-Yousef, M.M., Normal and respiratory variations of the hepatic and portal venous duplex Doppler waveforms with simultaneous electrocardiographic correlation. Journal of ultrasound in medicine, 1992. 11(6): p. 263-268.
Sivaciyan, V. and N. Ranganathan, Transcutaneous doppler jugular venous flow velocity recording. Circulation, 1978. 57(5): p. 930-939.
Tabata, T., J.D. Thomas, and A.L. Klein, Pulmonary venous flow by Doppler echocardiography: revisited 12 years later. Journal of the American College of Cardiology, 2003. 41(8): p. 1243-1250.
Hou, Y., et al., Clinical application of superior vena cava spectra in evaluation of pulmonary hypertension: a comparative echocardiography and catheterization study. Ultrasound in Medicine and Biology, 2016. 42(1): p. 110-117.
Ghio, S., et al., Doppler velocimetry in superior vena cava provides useful information on the right circulatory function in patients with congestive heart failure. Echocardiography, 2001. 18(6): p. 469-477.
Tremblay, J.-A., et al., Point-of-care ultrasonography to assess portal vein pulsatility and the effect of inhaled milrinone and epoprostenol in severe right ventricular failure: A report of 2 cases. A&A Case Reports, 2017. 9(8): p. 219-223.
Iida, N., et al., Clinical implications of intrarenal hemodynamic evaluation by Doppler ultrasonography in heart failure. JACC: Heart Failure, 2016. 4(8): p. 674-682.
Tang, W.W. and T. Kitai, Intrarenal venous flow: a window into the congestive kidney failure phenotype of heart failure? JACC: Heart Failure, 2016. 4(8): p. 683-686.