

Procalcitonin strategy in the ED did not reduce antibiotic use (ProACT)

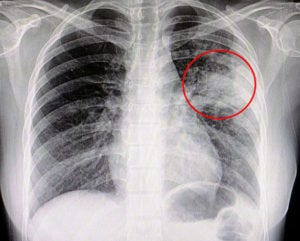
Procalcitonin-driven algorithms did not lead to lower antibiotic use for suspected pneumonias in the emergency department, in a large randomized trial. The multicenter ProACT trial enrolled 1,656 patients presenting with symptoms of pneumonia at multiple emergency departments. Patients were randomized to receive care guided by procalcitonin results (with thresholds to guide initiation or withholding of antibiotics), or usual care. Serial procalcitonin measurements were also provided to the medicine teams taking care of patients admitted from the ED with pneumonia. There was no difference in the average antibiotic days (4.2 vs. 4.3) between patients treated usually or with guidance from procalcitonin results. Poor clinical outcomes at 30 days were likewise similar between groups (11.7% for procalcitonin-guided vs 13.1% for usual care). Low or improving procalcitonin values appear useful as supporting evidence to help physicians discontinue antibiotics in hospitalized patients who are generally improving. Their main benefit is to reduce unnecessary antibiotic use. It's possible that using procalcitonin improves patient outcomes, but this is unproven. Procalcitonin has never been demonstrated to be sufficiently accurate for use as a stand-alone test to determine whether antibiotics should be provided for suspected infection. This study reinforces that point, and should discourage physicians from relying on procalcitonin levels over their clinical judgment when considering antibiotics for possible pneumonia in the ED. Infographic courtesy of visualmed.org:
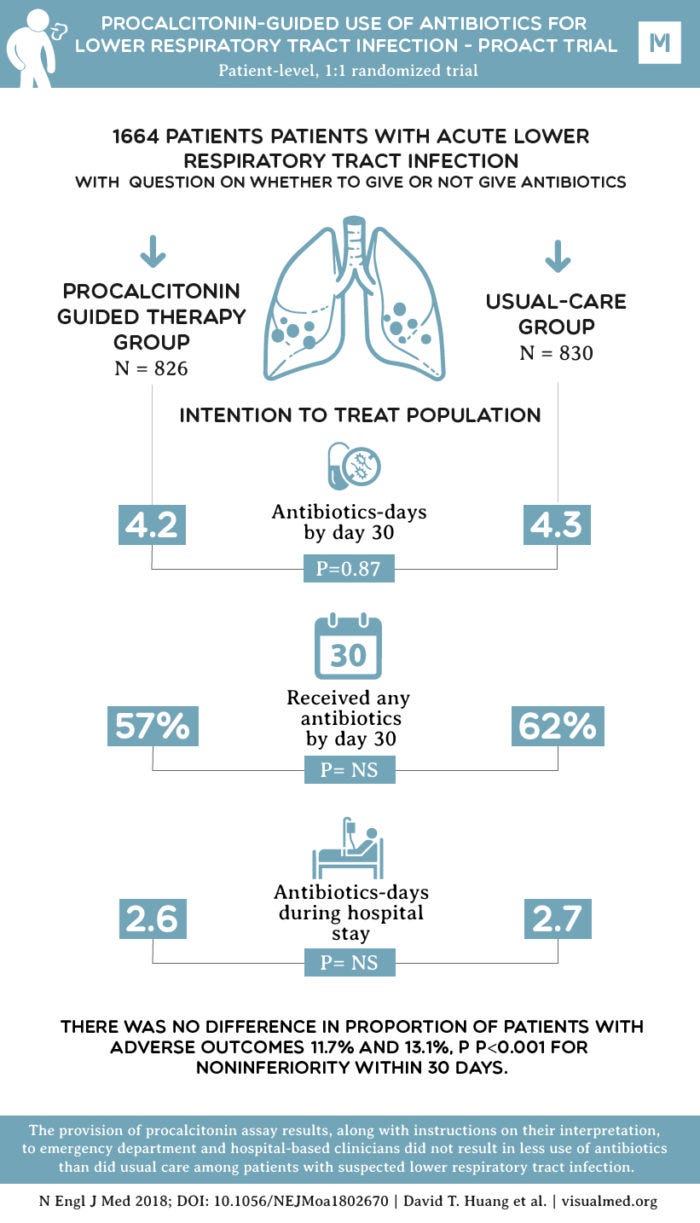
Source: NEJM