

The new "sepsis tests": do they work?
Part 2 of a series


There’s no diagnostic test for sepsis, which leads to high rates of overdiagnosis, delayed care from missed cases, and flawed clinical research.
Various new “sepsis tests” claim to solve the problem of diagnostic imprecision in the early management of suspected sepsis. Several have been FDA-cleared for sales and use in the U.S., and you may see them in your emergency department or ICU soon.
This series takes a closer look under the hood at these new tests, focusing on their methods and performance.
New "sepsis tests" are here: how well do they work?

Various new “sepsis tests” have come to market or will soon, claiming to solve the problem of diagnostic imprecision in the early management of suspected sepsis.
Today we’ll look at the newest market entrant: Triverity™, by Inflammatix™.
Triverity™
What Is It?
Triverity™ is a point-of-care blood test that measures the expression (mRNA) of genes associated with the immune system’s response to infection. Triverity was granted FDA’s 510k clearance in 2025, allowing the test to be sold commercially.
How it Works
A blood sample is placed in a cartridge and loaded into a small proprietary countertop machine. The “Myrna™” machine uses isothermal amplification (a cousin to PCR) to quantify mRNA sequences from 29 genes expressed during infections. Triverity™ does not identify pathogens or their genetic material.
Using AI/machine learning algorithms, a patient’s pattern of mRNA expression is indexed to previously observed patterns in patients with known bacterial or viral infections.
The algorithm returns results in one of five probability bands for bacterial or viral infection. The predicted severity of infection is also quantified.
Time to Results
About 30 minutes, according to Inflammatix.
How Was It Validated
Triverity™ was validated in 1,222 patients suspected to have acute infection with or without sepsis in 22 EDs (almost all in the U.S.)
No positive culture or other objective evidence for infection was required (at least as described in the preprint) to justify an adjudication of infection:
“First, without a true gold standard, we used clinical adjudication as the reference standard to determine the patient infection status.”
No data on rates of positive blood cultures, viral PCR results, etc. are reported in the preprint. Statuses of “bacterial infection”, “viral infection” or “no infection” were defined by the clinical opinion of two physician adjudicators, with a third acting as a tiebreaker, using available clinical data (including cultures, PCR, etc. if available).
The manuscript language refers to all the infections as if they were “true.” But in only 60% (n=729) could the two adjudicators reach an unforced consensus on who had infections or which kind. The other ~500 patients with equivocal infection status were then cherry-picked out to boost the top-line reported test performance. For the inflated performance using the smaller sample, read the preprint.
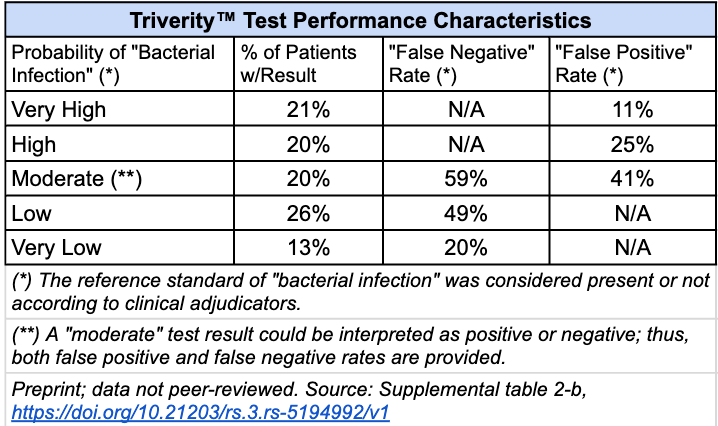
When all patients were included (results reported only in the supplemental material), Triverity’s five probability bands performed as follows:
Performance characteristics are highly influenced by the prevalence of the condition (infection, or the perception thereof, in this case), and the cutoff values chosen.
A surprisingly high 58% of patients were adjudicated to have bacterial infections; most presumed infections in EDs are viral, but only 20% were adjudicated as viral here. Only 19% of patients were adjudicated not to have had infections. The “true” infection rates are impossible to know.
The severity portion of Triverity™ had an AUROC of 0.77 (moderate discrimination) at predicting clinical deterioration:

According to Fierce Biotech, Inflammatix recently raised $57 million in anticipation of beginning its marketing efforts for Triverity™ after receiving FDA clearance. Inflammatix hasn’t reported any health systems using Triverity™, but the firm announced a new trial with a planned enrollment of 600 patients at EDs at Johns Hopkins and OSF Healthcare in Peoria, IL.
The (unfortunate) primary endpoints for the trial will be compliance with the SEP-1 bundle and time to final ED disposition order (admission or discharge).
But it won’t be a randomized controlled trial, nor fully prospective: after rolling out Triverity™ and collecting data on the experimental arm, a comparator (control) group will be fished from a retrospective database using propensity matching.
Discussion
Triverity™ avoids the pitfall of other “sepsis tests” that trap us in ontologic loops of uncertainty by calculating their own performance against a reference standard of “sepsis” defined by clinical criteria that do not require any evidence of infection.
Instead, it substitutes a different, but similarly fishy reference standard to validate its performance: the consensus opinion of clinical adjudicators as to whether a patient had a bacterial infection, a viral infection, or none. No objective data on whether infections were really present are provided in the preprint, which has yet to undergo peer review.
If the adjudicators’ powers of diagnosis and discrimination between bacterial and viral infections were perfect, Triverity™ missed 20% of the (adjudicated) bacterial infections at its most reassuring (“Very Low”) probability band. It underdiagnosed about half of the patients with a “Low” probability, ~49% of whom had adjudicated infections. (The higher performance reported in the paper was calculated by excluding the ~40% of patients with equivocal adjudication of their possible infections.)
Ruling out infections in lower-risk patients is much more important than ruling them in for higher-risk patients. Why? All patients had suspected infection as a condition of enrollment in the ED. The default will be that they will receive antibiotics, so a positive test is unlikely to change management; a false negative test could result in the dangerous withholding of antibiotics.
Yet because of the subjective reference standard, the level of certainty is low. For all anyone knows, the test was actually right 100% of the time and the adjudicators were wrong. How much faith should we place in their assessments, without knowing more about the patients, culture data, etc.?
Triverity™’s severity data was more interesting, being less tied to adjudicator assessments. It showed moderate discrimination in predicting which patients would need the ICU within 7 days.
But this would only be useful in cases where the potential for deterioration was not apparent already (e.g., to assist in triaging the right patients to monitored beds). We can’t tell that from the limited data provided.
Takeaway
Triverity™ uses amplification of mRNAs expressed by the immune system to predict the likelihood of bacterial or viral infections. It does not detect pathogens or their genetic material.
The validation study that led to its FDA clearance for sale and use in the U.S. has methodologic limitations (described above) that preclude any conclusions about the test’s real-world performance.
If we accept the study’s results at face value (i.e., assuming for the purpose of analysis that adjudicators’ assessments were always correct), Triverity™ performed poorly at ruling out bacterial infection in patients it classified as lower-risk.
Its severity prognostication appears to be more objective and moderately predictive of patient deterioration, but it’s impossible to tell how much additional discriminative power the test provides over clinical judgment.
Investors and hospital administrators may be impressed by Triverity™’s technology, but it will take more data to convince most practicing emergency physicians or intensivists of its value in making high-stakes decisions in patients with suspected infection.
My concern is that despite the poor performance of all of these "sepsis tests" there are outside interests that will push them to become "a standard of care."
Thank you for a series of posts.