

Tracheoinnominate artery fistula (Review)
A dreaded but rare complication, tracheoarterial fistulas elude systematic study

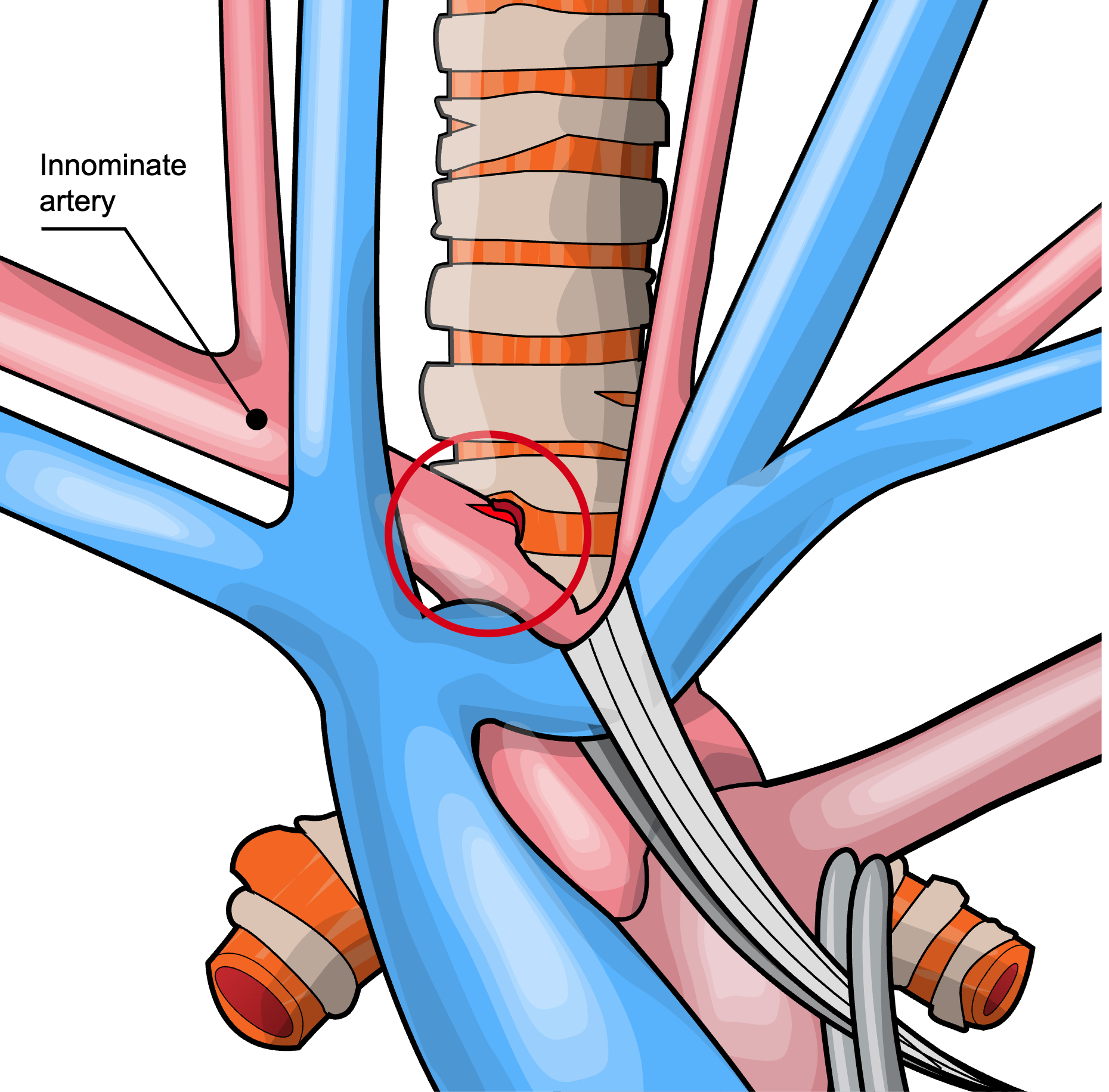
Fistulization between the trachea and the arterial system (usually by the innominate artery) is a dreaded complication of tracheostomy placement. This causes rapid bleeding into the airway that’s difficult to control, causing asphyxiation and/or exsanguination in minutes. In a case series of 137 patients published in the 1970s, the mortality rate was 92%.
Tracheoinnominate artery fistulae are uncommon, but their rarity has also made them difficult to study. Most literature has been reported as single-patient case series.
In a 2025 review of 148 published cases in 113 articles, Joshi et al provide valuable information about the diagnosis and management of tracheoinnominate artery fistulae.
For Bleeding ≥3 days Post-Trach, Suspect TIF
Bleeding from a tracheostomy is common and unlikely to represent a tracheoinnominate fistula, because they are fairly rare. The published incidence of TIF has been 0.7 to 1% after tracheostomy, but this is probably an overestimation. The true rate may be as low as 0.1% (1 in 1,000).
It has been reported that TIF may occur as soon as three days post-tracheostomy, with two-thirds occurring in the first three weeks. However, in reviews of published cases (which may be subject to publication bias), median time to TIF was two months.
Nevertheless, because the complication can be rapidly fatal, any bleeding more than a few days after tracheostomy should raise suspicion for TIF.
Bleeding from a TIF may present without warning as massive pulsatile arterial bleeding that floods the tracheobronchial tree in moments.
In 44% of reviewed cases, major bleeding was preceded by a sentinel hemorrhage. In about one-third of these, major bleeding followed within one day after a sentinel bleed; in another third, within 2 to 7 days; and one-third occurred later than a week after the herald bleed.
A pulsating tracheostomy tube, or bleeding that recurs with position changes, suctioning, coughing, or tube manipulation may be clues to the presence of a TIF.
What To Do For Suspected TIF
Overinflate the Tracheal Cuff Immediately
In 48 of 68 cases (71%) describing cuff overinflation, the maneuver was successful at controlling hemorrhage. Other series have reported 85% success rates with cuff inflation.
Call For Help
Pronounce a surgical emergency if TIF appears likely. Instruct staff to contact ENT, thoracic, vascular and general surgery. Activate the massive transfusion protocol.
Intubate Past the Tracheostomy
Endotracheally intubating past the tracheostomy and inflating the ET tube cuff distally can provide an additional barrier to blood flooding the airways.
Bronchoscopy via an endotracheal tube can also provide better access for suctioning of blood from the tracheobronchial tree, compared to rigid wand suction in the mouth or suction tubing inserted down the tracheostomy.
Compress the Innominate Artery
A finger inserted into the stoma and pulled inferiorly and anteriorly can compress the innominate artery. In the originally described Utley maneuver, the fascial plane anterior to the trachea is accessed with blunt dissection of the stoma, permitting finger entry into the pretracheal space and more direct compression of the artery.
Move to Definitive Management ASAP
Surgical and interventional radiology teams need to take over as soon as the patient can be moved to the OR or IR suites.
Open repair of the diseased innominate artery segment remains the traditional care standard. Median sternotomy and innominate artery ligation (division at the aortic arch and bifurcation) are generally performed.
Endovascular grafts and stents have been increasingly used as an alternative or temporizing measure.
Coil embolization of the innominate artery has also been described by interventional radiologists.
Mortality in more recently reported cases remains high: greater than 50%, but reduced from the historical 80-90%.
TIF Prevention
Tracheal cuff overinflation can cause mucosal injury and predispose to TIF. Cuff pressures no greater than 20 to 30 mmHg should be maintained.
For tracheostomy-associated bleeding suspected to be a sentinel TIF bleed, bronchoscopy should be performed.
CT scanning (ideally with contrast) may be more sensitive than bronchoscopy for developing TIFs that have not yet penetrated the tracheal mucosa.
TIF incidence has probably declined with the avoidance of low tracheostomy placements.
In accumulated case reports, percutaneous tracheostomy does not seem to be clearly associated with a higher (or lower) risk for the development of TIF.
References
Tracheo-Innominate Artery Fistula: A Systematic Review of Diagnostic and Management Strategies. Otolaryngology--Head and Neck Surgery : Official Journal of American Academy of Otolaryngology-Head and Neck Surgery. 2025. Joshi KD, Singh A, Singh DK, et al.
Tracheo-Innominate Artery Fistula After Percutaneous Tracheostomy: Three Case Reports and a Clinical Review. British Journal of Anaesthesia. 2005. Grant CA, Dempsey G, Harrison J, Jones T.
A Systematic Review of Mortality Associations in Patients Who Develop Tracheoinnominate Artery Fistula Following Tracheostomy. The American Surgeon. 2024. Ward K, Hinchman-Dominguez D, Stokes L, et al.
Tracheo-Innominate Fistula in Children: A Systematic Review of Literature. The Laryngoscope. 2019. Lee DJ, Yang W, Propst EJ, et al.
Pathological Consideration of Tracheo-Innominate Artery Fistula With a Case Report. International Journal of Pediatric Otorhinolaryngology. 2013. Miyake N, Ueno H, Kitano H.
Trachea-Innominate Artery Fistula: Retrospective Comparison of Treatment Methods. Southern Medical Journal. 1988. Yang FY, Criado E, Schwartz JA, Keagy BA, Wilcox BR.
Operative Technique for Tracheo-Innominate Artery Fistula Repair. Journal of Vascular Surgery. 2014. Furukawa K, Kamohara K, Itoh M, Morokuma H, Morita S.
Two Cases of Tracheoinnominate Artery Fistula Following Tracheostomy Treated Successfully by Endovascular Embolization of the Innominate Artery. Journal of Vascular Surgery. 2012. Hamaguchi S, Nakajima Y.
Sudden Death in a Rare Case Due to Tracheo-Innominate Artery Fistula. Journal of Clinical Medicine. 2024. Sacco MA, Gualtieri S, Longhini F, et al.