

What's the best method of weaning from mechanical ventilation?
FAST trial inadvertently reveals a crucial truth


After more than one hundred years of use, uncertainty persists as to the ideal way to wean (or “liberate”) patients from invasive mechanical ventilation (if any such ideal exists, that is).
Before extubation, a test of spontaneous breathing is performed, with either pressure-supported spontaneous breathing (in which the ventilator compensates for the difficulty of breathing through an endotracheal tube by delivering 8 cm H2O during each spontaneous breath, for example) or T-piece trials (in which the patient is disconnected from the ventilator circuit entirely, with high-flow oxygen flowing past the endotracheal tube tip).
Earlier trials suggested the use of protocols led to faster extubations, but there was no definitely superior method for predicting extubation success. Because pressure supported breathing is widely perceived as safer (owing to the ventilator’s backup modes and alarms possibly permitting earlier rescue of a failing patient) and more convenient (it can be performed with the touch of a few buttons without disturbing the ventilator circuit), it has almost completely supplanted the use of T-pieces during spontaneous breathing trials (SBTs).
Spontaneous breathing trials are conventionally performed once daily. It is unknown whether testing more than once a day might lead to faster liberation from mechanical ventilation.
A recent randomized trial sought to provide guidance on these two questions regarding SBT methods: is pressure-supported ventilation or T-piece superior, and is it better to attempt SBT once a day, or more frequently?
The Frequency of Screening and Spontaneous Breathing Trial Techniques (FAST)
Between 2018 and 2022, investigators led by the Canadian Critical Care Trials Group enrolled 797 mechanically ventilated patients at 23 ICUs in North America (receiving ≤70% FiO2 and PEEP ≤12 cm H2O), without tracheostomies, randomizing them to pressure-supported ventilation (with 0 to 8 and PEEP ≤5 cm H2O) or T-piece trials, and also to once-daily or more frequent screening for SBT readiness, in a 2 x 2 factorial design:
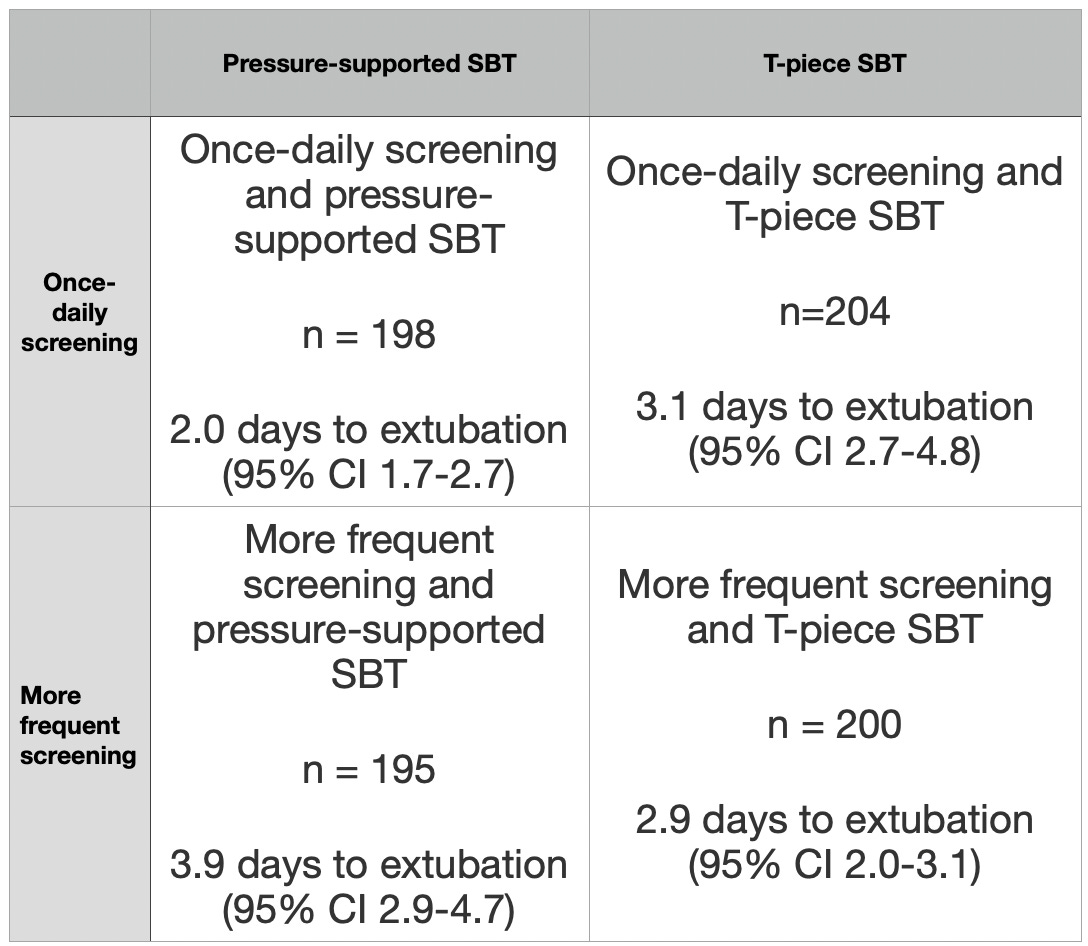
Patients randomized to once-daily screening with pressure-supported SBT (the conventional strategy) had the nominally shortest time to extubation: a median of 2.0 days.
Keep reading with a 7-day free trial
Subscribe to PulmCCM to keep reading this post and get 7 days of free access to the full post archives.