

2016 Surviving Sepsis Guidelines: A Review and Analysis

By Jon-Emile S. Kenny [@heart_lung] PulmCCM is not affiliated with or endorsed by the Society of Critical Care Medicine or the Surviving Sepsis Campaign. Click here to read the Surviving Sepsis Guidelines.
“I am at the moment writing a lengthy indictment against our century. When my brain begins to reel from my literary labors, I make an occasional cheese dip.”
-John Kennedy Toole
Collections of my favourite literary moments certainly occur in Toole’s posthumous masterpiece, A Confederacy of Dunces. Ignatius, a slovenly, quixotic character is often found lounging in his living room, belching and hollering at the ‘indecencies’ of mid-20th century television. He is incessantly writing his treatise on the vulgarities and hypocrisies that abound around him – until, of course, he is struck down by an unrelenting bout of peptic ulcer disease. While reading his exploits, I often wondered what kind of intensivist Ignatius would have been. Would he have had a blog? Twitter? Would he have been a protocol-pusher? An ardent algorithm adherent? With these musings, I turn to the new 2016 Surviving Sepsis Guidelines; and you’re in luck because I’ve just brewed a warm bowl of cheese dip.
New Definition
Firstly, there is the new definition of sepsis, as described here previously. In my view, we should avoid the 21st century lust for checklist-based medicine and the machismo of boasting on the size of one’s receiver operator curve. Let us, instead, focus on the new definition of sepsis: a life-threatening organ dysfunction caused by a dysregulated response to infection. Much of me wishes that the authors of sepsis 3.0 simplified the terminology as follows:
Presumed source + SIRS criteria = infection
Infection + life-threatening organ dysfunction = sepsis
Sepsis refractory to intravenous fluid = septic shock
We previously had no qualms about the imperfect definition of ‘severe sepsis.’ However, now that life-threatening organ dysfunction has been codified into bits and pieces of the SOFA score, it’s as if we’ve collectively lost our minds. Intensivists have formed opposing camps, each spying the other across desolate, evidence-based battlefields, desperately trying to lob another statistical grenade towards their hapless and misguided foe. Personally, I am satisfied that the sine qua none for the sepsis syndrome necessitates life-threatening organ dysfunction; it makes more sense.
Antibiotics & Initial Fluids
Once sepsis and septic shock have been identified, there remains a strong recommendation for early and broad parenteral antibiotics [within one hour] with appropriate source control. Interestingly, the authors make a distinction between sepsis and septic shock when considering empiric therapy [see recommendations 6 & 7 under antimicrobial therapy]. In those with septic shock [especially in those with a predicted mortality above 25%], it is recommended that ‘double coverage’ be employed – that is two antibiotics of different functional classes thought to target the pathogen of concern. By contrast, in those with sepsis or a predicted mortality of less than 15%, single coverage is recommended; this even applies to on-going therapy of sepsis with bacteremia, but without shock. However, the guidelines are clear that if multi-drug resistance is of concern, even patients with low predicted mortality should receive consideration for combination therapy and infectious disease consultation. The guidelines also encourage procalcitonin-based algorithms to assist in antimicrobial de-escalation; this usually requires trending procalcitonin values, so its level on presentation is prudent to obtain.
Importantly, and not unexpectedly, the Early Goal Directed Therapy [EGDT or ‘Rivers Protocol’] is no longer recommended based on the results of the ProMISe, ARISE and ProCESS trials. All of these large randomized controlled trials were published in 2014 and, essentially, torpedoed the original Rivers protocol. The authors do correctly note that there was no harm in the EGDT arm of the big 3 trials, so it is not incorrect to follow the classical, EGDT pathway. Instead, however, for initial resuscitation, the authors suggest 30 mL/kg of crystalloid [saline or balanced] upfront and within 3 hours of diagnosis. No longer are the days of targeting a central venous pressure [CVP] of 8-12 mmHg. Instead of the CVP, the authors currently, and correctly, identify the use of dynamic variables for assessing fluid responsiveness. This does not diminish my appreciation for the physiology of the CVP; its genesis must still be understood just as one knows the determinants of the stroke volume. Importantly, knowing the origins of the CVP makes clear why its static value should never have been used as a marker of volume status or volume responsiveness.
Critically, whilst not specifically noted within the guidelines, not all dynamic variables are created equal. Given the variability of cardiorespiratory pathologies in the intensive care unit, the most universally applicable dynamic assessments demand an increase in venous return [e.g. passive leg raise, mini fluid challenge, end-expiratory occlusion test] followed by an immediate measurement of left ventricular output [e.g. esophageal Doppler monitoring]. Moreover, given the large proportion of patients who are fluid non-responsive in the ICU, blindly giving 2-3 L of crystalloid upfront is, potentially, disastrous. In patients with known, underlying cardiac disease [plus a brewing septic cardiomyopathy], it may be wise to assess fluid responsiveness early and often.
The issue of albumin or crystalloid was also addressed with recommendation for the latter during initial resuscitation. The authors detail the handful of meta-analyses comparing albumin to crystalloid since the 2012 guidelines, additionally they make note of the ALBIOS trial. In the former analyses, there were trends towards improved mortality in those who received albumin, typically in more ill patients – i.e. those in shock – but there was mixed data as well. Notably, in ALBIOS, albumin tended to normalize hemodynamics earlier and reduce volume needs, but this trial targeted fluid resuscitation over 28 days, making its application to acute resuscitation difficult. In summation, the current guidelines recommend albumin as resuscitation in addition to crystalloids, only if ‘substantial’ crystalloid is required.
Blood Pressure & Vasoactives
The guidelines carefully dissect the target mean arterial pressure [MAP] thoughtfully. The consensus is to target 65 mmHg MAP despite subgroup analysis of the SEPSISPAM trial revealing that chronic hypertension patients may have less renal dysfunction if a higher MAP is achieved. Targeting a higher blood pressure was tempered against increased arrhythmia risk and – in one small trial – increased mortality in the elderly.
The current guidelines recommend norepinephrine as the vasoactive medicine of first choice in sepsis and septic shock. As compared to dopamine, norepinephrine has been demonstrated in a large meta-analysis to be superior; whereas, when norepinephrine is compared to epinephrine, no clear difference in outcome was observed. The authors also undertook their own meta-analysis to compare norepinephrine to vasopressin, which included the recent VANISH trial. No difference was found between the two vasoactive medications and this held true even when studies which combined norepinephrine and vasopressin were excluded from the analysis. Given the aforementioned, both vasopressin and epinephrine are regarded as ‘second-line’ considerations following the initiation of norepinephrine. Dopamine should be used only in highly selected patients with very low risk of tachyarrhythmias. There is no strong recommendation dobutamine unless the patient is persistently hypoperfused despite adequate intravascular volume repletion and vasoactive medication infusion. The guidelines also note the findings of the CATS trial which showed no difference in outcome between norepinephrine and dobutamine as compared to epinephrine. Epinephrine does, however, raise lactate levels via B2 adrenergic receptor stimulation. Accordingly, if epinephrine infusion is utilized, a rising lactate level should not be taken as evidence of ‘hypo-perfusion’ but rather, adrenergic stress – which is, in my opinion, the most common cause of lactate elevation worldwide.
Lactate
The authors make recommendation number 7 under initial resuscitation: ‘normalize lactate in patients with elevated lactate levels as a marker of tissue hypo-perfusion;’ they grade this as a weak recommendation, low quality of evidence. Interestingly, buried within the text they declare - correctly - that ‘serum lactate is not a direct measure of tissue perfusion.’ So why the emboldened recommendation that lactate is the messenger of tissue starvation? In my opinion, the importance of lactate is probably that it serves as a cognitive reminder to give fluids early – even if the reasoning for the fluids is misguided. A falling lactate in response to preload does not necessarily imply improved tissue oxygenation; it may actually reflect a fall in adrenergic tone – just as heart rate falls in response to intravenous fluids.
Other Recommendations
The issue of corticosteroids in sepsis and septic shock continues to wax and wane with different pieces of evidence supporting or refuting their use in various patient populations under equally diverse dosing protocols and durations of therapy. Ultimately, the guidelines suggest, weakly, that 200 mg of hydrocortisone, daily, be administered in patients with septic shock refractory to fluids and vasoactive infusions. Further, the guidelines go on to provide a recommendations for a variety of sepsis-related management concerns including: mechanical ventilation, blood glucose control, nutrition, blood products, immunoglobulins, sedation, analgesia and much more.
Below is my own cognitive algorithm that I created from the new guidelines, but these topics go far beyond this brief reflection. Please check out these meaty guidelines yourself, and – may I humbly suggest – do so over a savoury cheese dip; be like Ignatius.
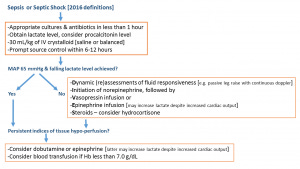
Summary Figure: please note that this figure represents my personal interpretation; it should not be used to replace a clinician's independent evaluation of the Society of Critical Care Medicine's Surviving Sepsis Guidelines.
Lastly, physiology learning module 6 is now live!
Happy Birthday Dr. Miyakawa, JE
PulmCCM is not affiliated with or endorsed by the Society of Critical Care Medicine or the Surviving Sepsis Campaign. Views and commentary above are solely the author's.