

ICU Physiology in 1000 Words: Fighter Pilots!

Jon-Emile S. Kenny MD [@heart_lung] with illustrations by Carla M. Canepa MD
Pilots of high-performance, tactical fighter jets each have continuous positive airway pressure [i.e. CPAP] masks as a part of their flight suit. Strikingly, beyond the clinically-commonplace airway pressure of 5-15 cm of H2O, a fighter pilot may endure a mask-applied pressure of 90 cm H2O [1]! How and why is this physiology acceptable? Is there any clinical relevance?
+Gz - Associated Loss of Consciousness
The abbreviation +Gz refers to a head-to-foot inertial force resulting from an equal but opposite acceleration [2] see figure 1. Inertial forces in this direction occur, for instance, when an aircraft is rapidly directed upwards from a deep dive. More simply, think of organs and tissues - including blood - moving downwards at high velocity; when there is a rapid, upwards correction of the aircraft, an inertial force in the +Gz axis keeps all tissue, including blood, moving downwards against the will of the aircraft.
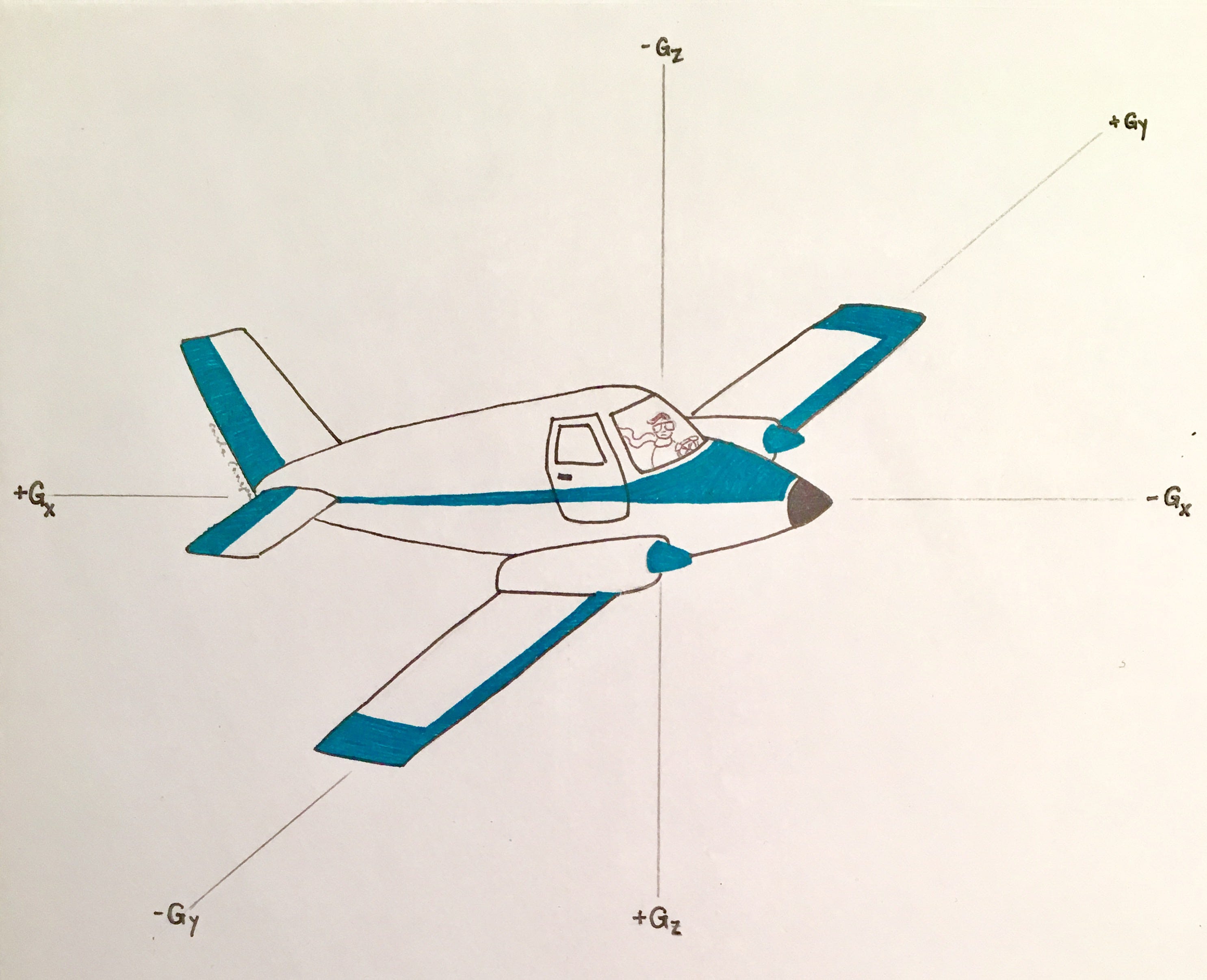
Figure 1: x, y and z axes depicting forces in aviation medicine. The +Gz axis is directed in the head-to-foot direction
An increase in G force to twice that of gravity, i.e. +2Gz, results in a 20-25 mmHg reduction in mean arterial pressure [MAP] at the level of the head [2]. This reduction in MAP holds for each additional increment in G force such that at +4Gz, the MAP at the level of the head will fall by roughly 100 mmHg. Accordingly, the typical +Gz level tolerated by relaxed humans is about +3.5Gz before there is +Gz - associated loss of consciousness, or GLOC [3]. Perhaps the first description of GLOC was nearly a century ago in an esoteric chapter entitled “Sensations Experienced by Normal Persons in Machines Heavier than Air” [4].
Fundamentally, GLOC is secondary to cerebral hypoperfusion which has been evaluated via various methods including transcranial Doppler [5]. Indeed, there is a dose-dependent reduction in middle cerebral artery flow with increasing +Gz and in subjects with GLOC, reversal of MCA flow was noted! Of interest, the moment of GLOC is not simultaneous to cessation of cerebral blood flow but rather lags by by 5 - 10 seconds; this delay is known as the cerebral anoxic reserve [6] - first systematically studied in healthy, young prisoners in the mid-20th century [7].
Prevention of GLOC: Anti-G suits
Basic hemodynamics and heart-lung interaction are exploited in modern aircraft to augment the level and duration of +Gz tolerance. Fighter pilots can now readily withstand up to +12 Gz! From the reduction of cerebral pressure described above, maintenance of cerebral perfusion at +12 Gz [assuming a cardiac-to-head distance of 30 cm & a seat at 30 degrees from the vertical] demands a left ventricular pressure approaching 300 mmHg [2]. Such pressure can be achieved via the use of Anti-G Suits [AGS], positive pressure breathing for +Gz tolerance [PBG] and the Anti-G straining maneuver [AGSM] [1].
Initially, attempts to maintain high cardiac pressure in the face of +Gz force focused on augmenting venous return [6]; this included the first AGS used in combat - invented by Wilbur Franks. Contemporary AGS apply compression pressures that eclipse 200 mmHg to the extremities and abdomen in response to high +Gz [2, 8]. Mechanistically, wrapping of the veins intensifies venous return [9]; further, mechanical restraint of the arteries increases peripheral arterial resistance directing arterial blood to the head [1]. Lastly, abdominal compression by the AGS physically raises the heart [10] which lowers the pressure gradient to the cerebral circulation.
Venous return and arterial resistance are also enhanced by +Gz training, for example in a centrifuge. Fighter pilots have decreased venous capacitance; that is, have a higher venous pressure for a given blood volume and they are more sensitive to phenylephrine infusion compared to normal controls [11]. It is, therefore, presumed that their enhanced +Gz tolerance is mediated by alpha-receptors [11].
Prevention of GLOC: Positive pressure breathing for +Gz tolerance
The application of high airway pressure, as described in the introductory paragraph, also enhances cerebral perfusion by squeezing arterial blood out of the left ventricle and thorax [12]. The COMBAT-EDGE system administers 16 cm H2O of airway pressure for each +Gz above 4 to a maximum of 82 cm H2O at +9Gz [13]. While airway pressure of this degree may concern clinicians, high +Gz force simultaneously raises chest wall weight thereby limiting the trans-pulmonary pressure, or distending pressure of the lung [14]. This is akin to the morbidly obese in the ICU with high airway pressure. Additionally, some flight suits splint the chest wall by inflating a bladder around the anterior chest to the same level as pressure applied to the airway, though this may be redundant [14].
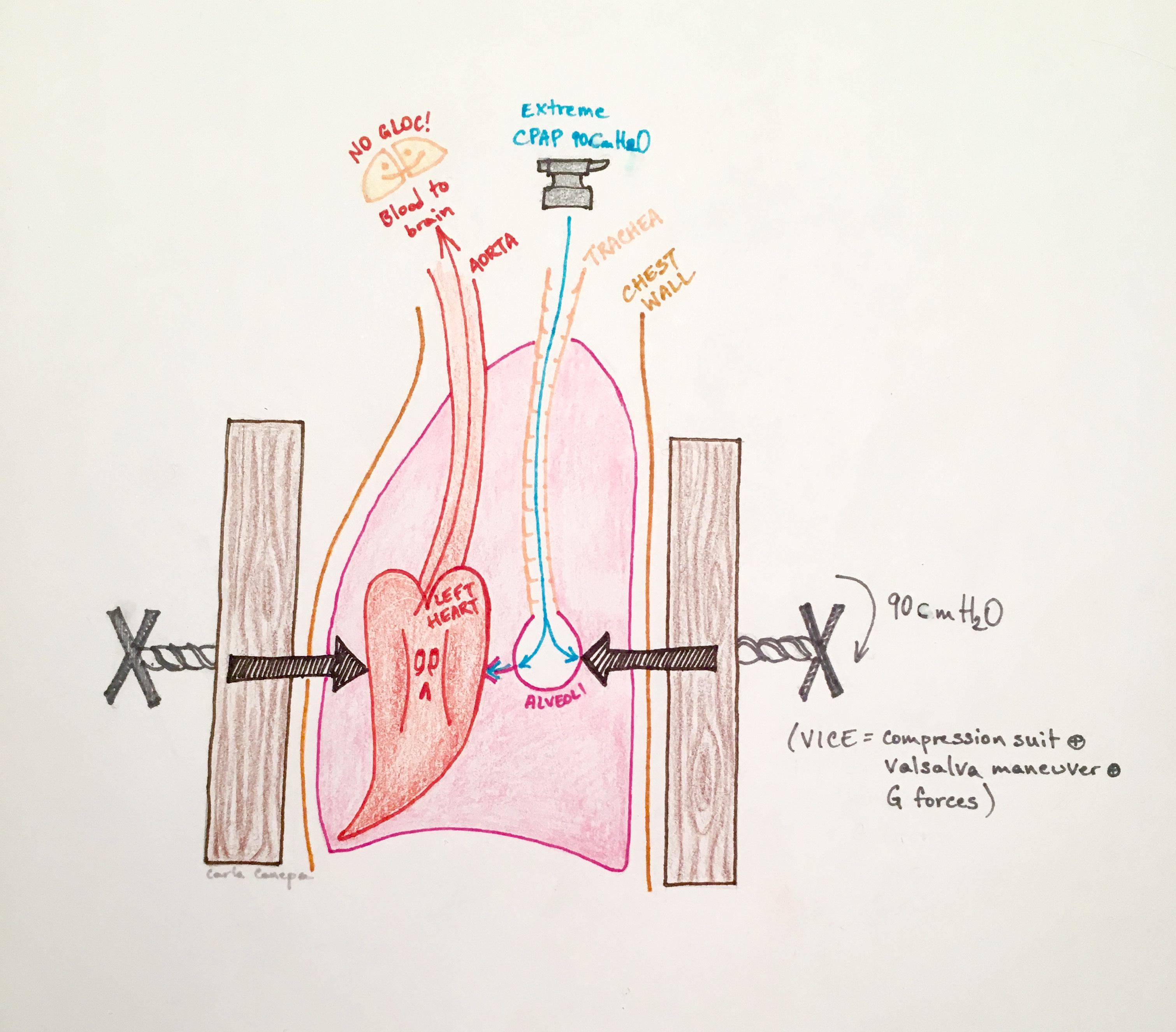
Figure 2: Cartoon depicting PBG. The application of extreme CPAP [the anvil] in the setting of a stiffened chest wall [the vice]. Note that the distending pressure across the alveolus or trans-pulmonary pressure is not extreme because of the stiffened chest wall. Also, the increase in pleural pressure enhances left ventricular ejection of blood.
Prevention of GLOC: Anti-G straining maneuver
As a supplement to PBG, pilots routinely perform strenuous maneuvers comparable to valsalva, interspersed with breaths. Additionally, clenching of muscles in the extremities are performed to maintain venous return and raise arterial pressure. Collectively, the aforementioned is termed the anti-G straining maneuver [AGSM]. The AGSM has been shown to increase +Gz tolerance by 2-3 with measured esophageal pressure [Pes, surrogate for pleural pressure] up to 140 cm H2O [or 100 mmHg] [15].
Clinical Relevance
Perhaps the most important concept highlighted by the extreme physiology of high +Gz is that of the pressure across a distensible structure, or the trans-mural [Ptm] pressure. The Ptm makes clear that it is not simply the pressure inside the object [e.g. airway pressure], but rather it is the pressure inside relative to the outside [i.e. airway pressure relative to pleural pressure] that is physiologically meaningful. In a fantastic study [8] of volunteers receiving extraordinary CPAP - with both pulmonary arterial and esophageal catheters in place - the Pes was higher than the applied airway pressure of 95 cm H2O. In other words, the Ptm fell and lung volume shrunk in the volunteers wearing chest wall counter-pressure. This is also why airway pressure may reach 200-300 mmHg during coughing [16, 17].
Additionally, the measured mean pressure in the pulmonary artery rose to 77 mmHg! However, this did not increase the afterload of the right ventricle; the trans-mural pressure of the pulmonary artery actually fell [8], meaning that RV outflow impedance also fell.
In the face of such high intra-thoracic pressure, the importance of venous return is also highlighted, both by intrinsic adrenergic tone and externally-applied AGS which increase the mean systemic pressure and drive venous blood to the right heart.
Lastly, there is one more interesting parallel between high +Gz physiology and the ICU; the prone position is a protective posture. Pronation of a fighter pilot in the cockpit would nullify the +Gz pressure gradient from the heart to the head [18], effectively abolishing GLOC.
Please check out other posts in this series,
p.s. good luck on the pulmonary boards today, Dr. Miyakawa!
References
Lauritzsen, L.P. and J. Pfitzner, Pressure breathing in fighter aircraft for G accelerations and loss of cabin pressurization at altitude—a brief review. Canadian Journal of Anesthesia/Journal canadien d'anesthésie, 2003. 50(4): p. 415-419.
Burns, J.W., et al., Protection to+ 12 Gz. Aviation, space, and environmental medicine, 2001. 72(5): p. 413-421.
Parkhurst, M., S. Leverett Jr, and S. Shubrooks Jr, Human tolerance to high, sustained+ G z acceleration. Aerospace medicine, 1972. 43(7): p. 708-712.
Burton, R.R., G-induced loss of consciousness: definition, history, current status. Aviation, space, and environmental medicine, 1988.
Ossard, G., et al., Response of human cerebral blood flow to+ Gz accelerations. Journal of applied physiology, 1994. 76(5): p. 2114-2118.
Wood, E.H., Prevention of the pathophysiologic effects of acceleration in humans: fundamentals and historic perspectives. IEEE Engineering in Medicine and Biology Magazine, 1991. 10(1): p. 26-36.
Smith, B.A., E.W. Clayton, and D. Robertson, Experimental arrest of cerebral blood flow in human subjects: the red wing studies revisited. Perspectives in biology and medicine, 2011. 54(2).
Balldin, U. and B. Wranne, Hemodynamic effects of extreme positive pressure breathing using a two-pressure flying suit. Aviation, space, and environmental medicine, 1980. 51(9 Pt 1): p. 851-855.
Burns, J.W., M.J. Parnell, and R.R. Burton, Hemodynamics of miniature swine during+ Gz stress with and without anti-G support. Journal of applied physiology, 1986. 60(5): p. 1628-1637.
Rushmer, R.F., A roentgenographic study of the effect of a pneumatic anti-blackout suit on the hydrostatic columns in man exposed to positive radial acceleration. American Journal of Physiology--Legacy Content, 1947. 151(2): p. 459-468.
Convertino, V.A., High sustained+ Gz acceleration: physiological adaptation to high-G tolerance. Journal of gravitational physiology: a journal of the International Society for Gravitational Physiology, 1998. 5(1): p. P51-4.
Buda, A.J., et al., Effect of intrathoracic pressure on left ventricular performance. New England Journal of Medicine, 1979. 301(9): p. 453-459.
Travis, T.W. and T.R. Morgan, US Air Force positive-pressure breathing anti-G system (PBG): subjective health effects and acceptance by pilots. Aviation, space, and environmental medicine, 1994. 65(5 Suppl): p. A75-9.
Grönkvist, M., et al., G tolerance and pulmonary effects of removing chest counterpressure during pressure breathing. Aviation, space, and environmental medicine, 2005. 76(9): p. 833-840.
Eiken, O., et al., G protection: interaction of straining maneuvers and positive pressure breathing. Aviation, space, and environmental medicine, 2007. 78(4): p. 392-398.
Sharpey-Schafer, E., The mechanism of syncope after coughing. British medical journal, 1953. 2(4841): p. 860.
Green, N., Lung volumes during+ Gz acceleration and the effects of positive pressure breathing and chest counter-pressure. Journal of gravitational physiology: a journal of the International Society for Gravitational Physiology, 1994. 1(1): p. P41.
Wood, E., Operational requirements for avoidance and eventual elimination of Gz-induced loss of consciousness (G-LOC) in flight. The Physiologist, 1993. 36(1 Suppl): p. S106.