

ICU Physiology in 1000 Words: The Mean Systemic Filling Pressure – Part 1

Jon-Emile S. Kenny MD [@heart_lung]
It’s 4 in the morning; I am somewhere between Riga and Stockholm. The moon is full and bright and rippling across the black, Baltic Sea. This warm, June darkness is cut like onyx by deep vibrations of a cruise ship and its collections of giggling Swedes; they karaoke ‘Spaceman’ by The Killers in perfect English. I’m perched portside, caught in a yawning ocean breeze, surrounded by a symphony of Slavic slangs and cigarette smoke; my mind turns to the innards of the ship and I imagine a physiological analogy.
The Hull as the Thorax
Consider sitting deep within the hull of this cruise ship, ignorant to the outside. A leak is sprung and ocean begins to rush in. Thinking quickly you activate the bilge pump which, appropriately, ejects the ocean outside again. You note that the bilge pump has a number of settings from ‘low’ to ‘high’ corresponding to the rate at which it evacuates ocean from inside the hull. When the pump’s setting is ‘low,’ ocean water rises inside the hull – you feel the water’s pressure around your ankles. When you increase pump activity to ‘high,’ the pressure and volume of ocean water around your feet abate. Knowing only this, can you infer the size of the body of water beyond the hull? Are you in the relatively small Baltic or the immense Pacific? Lake Ontario? The Hudson River? Wreck Beach?
The answer is that you cannot know; the amount of ocean water within the hull of the ship is a function of the size of the body of water outside of the hull and its inflow, but also on the efficacy of the bilge pump. Thus, the analogy unfolds – we have approximated volume status [the vastness of the ocean], venous return [the ocean rushing into the boat], the thorax [the hull of the boat], the heart [the bilge pump] and the central venous pressure, great vein and cardiac chamber volume [the pressure and volume of the ocean water accumulating within the hull of the boat].
Yet, I continue to see clinicians use right atrial pressure, IVC volume/collapse and echocardiographically-measured left ventricular volume as markers of a patient’s volume status. Looking only into the thorax for patient’s volume status is as preposterous as estimating the size of an ocean based on the amount sea water accumulating within the hull of a leaky ship.
Volume Status & Venous Return
Approximately 70% of the total blood volume lies within the venous system, another 20% in the arterial system and about 10% in the capillaries [1]; this total blood volume can be estimated as 70-80 mL/kg. When the heart is stopped and blood volume distributes itself from the poorly compliant, high pressure arteries, to the highly compliant, low pressure veins, an equilibrium pressure is achieved known as the mean systemic filling pressure [Pmsf]. The value of the Pmsf is typically between 7 and 10 mmHg and independent of species and habitus [1-3]. This pressure is a function of the stressed ‘volume status’ of the patient and venous compliance; it is the pressure head driving venous return towards the right heart. On the venous return curve, this pressure is marked by the x-intercept, because this is the equilibrium pressure that persists throughout the circulation when blood flow [y-axis] is zero.
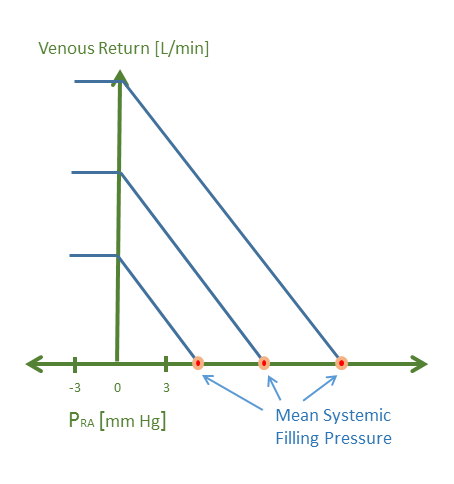
Figure 1: Venous return curves at 3 different mean systemic pressures; this may represent 3 different blood volume states e.g. hypo-, eu- and hypervolemic. Venous return is on the y-axis and right atrial pressure on the x-axis. When venous return is zero, right atrial pressure equals the mean systemic filling pressure [Pmsf]. The Pmsf is determined by both the stressed vascular volume and venous compliance.
The notion of stressed volume may be thought of analogously to that of a water bed, or inflating a beach ball. A certain volume of fluid must be added before the elastic walls are stretched – this volume is the unstressed volume. When the volume of fluid added begins to stretch the walls, an elastic recoil pressure is generated. Accordingly, the volume that contributes to this elastic recoil is known as the stressed volume. In humans undergoing hypothermic, circulatory arrest, the stressed volume was estimated to be about 20 mL/kg or about 1.5 L of blood volume [4]. Importantly, the stressed volume is not fixed, and highly dependent upon adrenergic tone, especially alpha-adrenergic tone [5]. Thus, the Pmsf is directly, but not wholly, related to a patient’s overall blood volume.
Measuring the Mean Systemic Filling Pressure
If we desire to know the size of the ocean, we must look beyond the hull of the thorax; is there a way to measure the Pmsf? Firstly, as above, one can stop the heart and allow the pressures in the arteries, veins and heart equilibrate to the Pmsf. This has been attempted in patients who have died in the ICU, as well as in patients undergoing fibrillatory arrest prior to the placement of a defibrillator [6, 7]. In a recent analysis, Repesse and colleagues found the Pmsf to be 13 mmHg +/- 5.5 mmHg, 1 minute following clinical death [6]; as above, because alpha-adrenergic tone plays a key role in the fraction of the stressed blood volume, norepinephrine infusion before death was associated with a higher Pmsf. Interestingly, fluid balance was not associated with Pmsf following death which may reflect the importance of vascular tone in determining Pmsf and the plethora of interventions which alter the adrenergic system [e.g. sedation, vasopressors, steroids, mechanical ventilation etc.] within the ICU. As elaborated by Rothe [8], a range of Pmsf may be seen at any given volume status all as a function of degree of adrenergic tone. In this data, euvolemia can see a Pmsf vary between ~7 and 14 mmHg depending upon absence or presence of adrenergic activity, respectively.
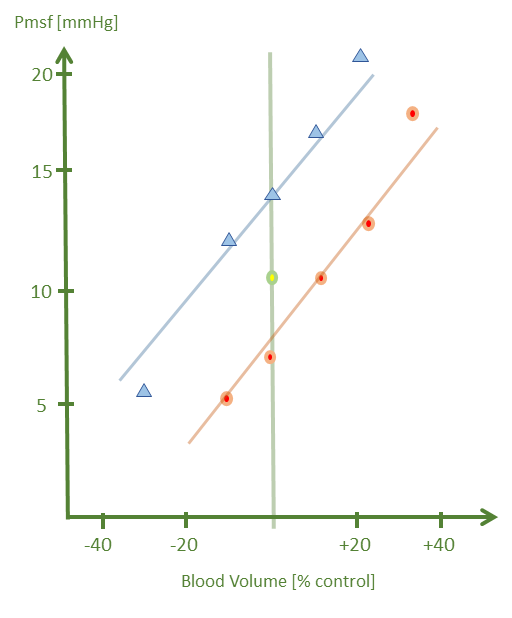
Figure 2: Blood volume on the x-axis and Pmsf on the y-axis. The green line bisecting the graph represents euvolemia or 100% blood volume. The blue line/triangles represent the effect of norepinephrine while the orange line/circles represent adrenergic blockade. Note that a given blood volume on the x-axis can have a range of Pmsf depending on vascular tone. The green circle in the middle represents the control condition [i.e. 100% blood volume with baseline adrenergic activity].
While cessation of cardiac activity is considered the gold-standard for measuring Pmsf, it is clearly not feasible clinically. Fortunately, there are three other methods of approximating the Pmsf which do not require cardiac arrest; these methods are described in more detail in part 2.
Please check out more posts in this series,
References
Aya, H.D. and M. Cecconi, Can (and should) the venous tone be monitored at the bedside? Current opinion in critical care, 2015. 21(3): p. 240-244.
Magder, S., Bench-to-bedside review: An approach to hemodynamic monitoring - Guyton at the bedside. Crit Care, 2012. 16(5): p. 236.
Starr, I., Role of the" static blood pressure" in abnormal increments of venous pressure, especially in heart failure. ii. clinical and experimental studies. The American Journal of the Medical Sciences, 1940. 199(1): p. 40-54.
Magder, S. and B. De Varennes, Clinical death and the measurement of stressed vascular volume. Crit Care Med, 1998. 26(6): p. 1061-4.
Gelman, S., Venous function and central venous pressure: a physiologic story. Anesthesiology, 2008. 108(4): p. 735-48.
Repessé, X., et al., Value and determinants of the mean systemic filling pressure in critically ill patients. American Journal of Physiology-Heart and Circulatory Physiology, 2015. 309(5): p. H1003-H1007.
Schipke, J., et al., Static filling pressure in patients during induced ventricular fibrillation. American Journal of Physiology-Heart and Circulatory Physiology, 2003. 285(6): p. H2510-H2515.
Rothe, C.F., Physiology of venous return. An unappreciated boost to the heart. Arch Intern Med, 1986. 146(5): p. 977-82.