

ICU Physiology in 1000 Words: Heliox & Mechanical Power

Jon-Emile S. Kenny MD [@heart_lung]
Of the countless things taught to me by Dr. Chitkara at the Palo Alto VA Health Care System, one that sticks is the difference between density-dependent and viscosity-dependent airflow. He often used the chronic bronchitic suffering through the viscous, humid New York City summers as a teaching example. The importance of gas density and viscosity is also frequently encountered when considering the properties and benefits of helium-oxygen gas mixtures [i.e. ‘Heliox’]. This brief review highlights the viscosity and density characteristics of gas within the context of the mechanical power applied to the lung; as such, roles for Heliox may extend beyond that of a rescue therapy for severe obstructive airways disease.
Mechanical Power
As outlined in this previous post on ARDS, Cressoni and colleagues have proposed a fascinating approach to minimizing ventilator-induced lung injury [VILI] [1]. Instead of focusing solely upon the static or elastic properties of the respiratory system [i.e. minimizing lung volume and plateau pressure], they argue that mechanical power should be the variable of interest. The implication is that the clinician should concentrate not only upon lung volume and plateau pressure, but also upon the peak pressure [i.e. the dynamic or resistive properties] and the respiratory rate – for it is all of these variables which determine the mechanical power applied to the lung skeleton [see Figure 1].
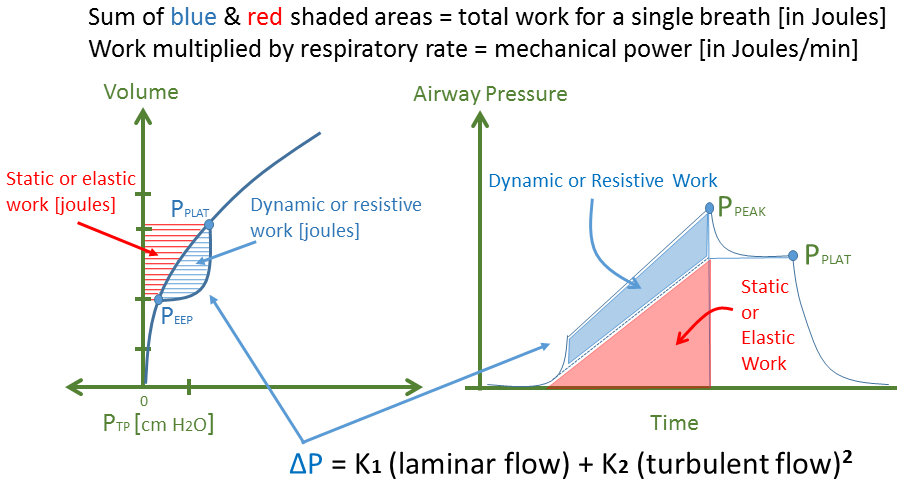
Figure 1: The left portion of figure 1 reveals the work applied to the lung, parsed into its static [red] and dynamic [blue] components. The left figure is modified from classic physiology diagrams such as the Rahn diagram. If pressure is moved from the x-axis to the y-axis and volume is moved from the y-axis and changed to time on the x-axis, the clinically-relevant ventilator waveform can be visualized on the right. Importantly, volume can become time only if flow is constant [i.e. square wave delivery]; constant flow means that the same volume is delivered per unit time, in other words, volume and time become linear analogs. Also, the ventilator waveform represents not the Ptp but the pressure across the respiratory system in the passive patient. If esophageal pressure were subtracted from the airway pressure, Ptp would be obtained. Ptp is transpulmonary pressure; Ppeak is peak pressure; Pplat is plateau pressure; Peep is positive end-expiratory pressure; ΔP is the dynamic pressure gradient [blue].
If the model of Cressoni and colleagues proves true, it may be prudent to minimize the dynamic properties [blue shaded] of the pulmonary pressure-volume relationship in an effort to mitigate VILI. The magnitude of the dynamic pressure applied to the effortless, mechanically-ventilated patient can be simplified to the equation at the bottom of figure 1; that is, the pressure [ΔP] required to drive both laminar and turbulent airflow [2]. For simplicity, this analysis neglects ‘transitional’ airflow which lies between laminar and turbulent airflow in its effects on dynamic pressure.
Physiology of Helium-Oxygen Mixtures
Replacing nitrogen with helium has two effects on gas properties. Firstly, because helium is much less dense than nitrogen, Heliox is considerably less dense than air. Secondly, and often neglected, is that helium is slightly more viscous than nitrogen, consequently, Heliox is mildly more viscous than air [2, 3]. As illustrated in figure 2, these differences in density [p] and viscosity [u] have complicated and somewhat conflicting effects upon the pressure required [ΔP] for a given ventilator-applied gas flow.
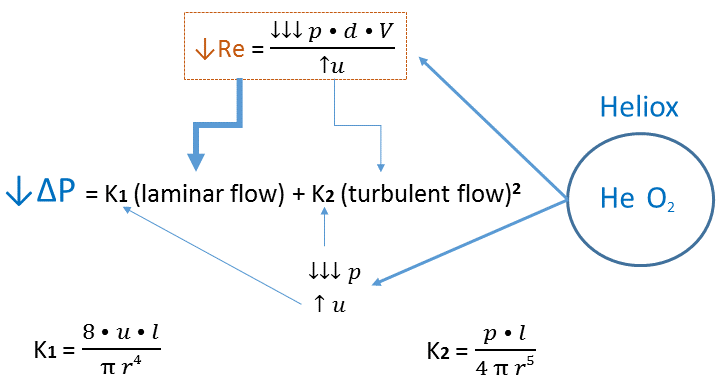
Figure 2: Re is Reynold's Number; p is gas density; d is tube diameter; V is gas velocity; u is gas viscosity; l is tube length; r is tube radius; ΔP is the dynamic pressure gradient. Heliox diminishes gas density to a larger degree than it raises gas viscosity [see text].
Heliox reduces Reynold’s Number [Re] which is the ratio of inertial forces [density-dependent, viscosity-independent] to viscous forces [viscosity-dependent, density-independent] in a perfect tube [3]. The lower the Re, the more likely laminar flow is to occur, while the higher the Re, the more likely turbulent flow is to occur. In figure 2, the lower Re is shown to create a larger fraction of laminar flow as depicted by the emboldened arrow towards laminar flow. This effect has a large reduction in ΔP because it is the square of turbulent airflow that is proportional to ΔP.
Yet Heliox has direct effects upon the laminar and turbulent flow which exists within a given Re milieu. As can be seen by the constants which mediate laminar [K1] and turbulent [K2] airflow, the reduced density of Heliox lowers K2 such that ΔP is reduced, but Heliox slightly increases K1 because of the small increase in viscosity. It should not escape the reader that both K1 and K2 are highly and inversely related to the radius of the airway through which gas flows [2]. Thus, airway caliber also plays a pivotal role in the resistive ΔP value.
Inspiratory Effects
The effect of Heliox on peak inspiratory pressure [Ppeak] has been demonstrated in a number of trials of obstructive airways disease. Indeed, in one small study a dramatic reduction in the mean Ppeak by 32 cm H2O was found [4]. Additionally, Lee and colleagues found a 10 cm H2O reduction in Ppeak [5] and Tassaux et al. noted an average fall in Ppeak by 5 cm H2O [6]. While the differences between these trials may be related to severity of disease, fraction of helium utilized as well as tidal volume and flow delivered, there is a consistent finding that in the effortless, ventilated patient, Heliox reduces dynamic, inspiratory pressure. The overall effect is to drop resistive work and therefore mechanical power.
Expiratory Effects
In addition to a consistent Heliox-induced fall in Ppeak, there is also a fairly reliable reduction of intrinsic positive end-expiratory pressure [PEEPi]. Expiratory flow through an obstructed airway can be modeled with the orifice flow equation [see figure 3] [2].
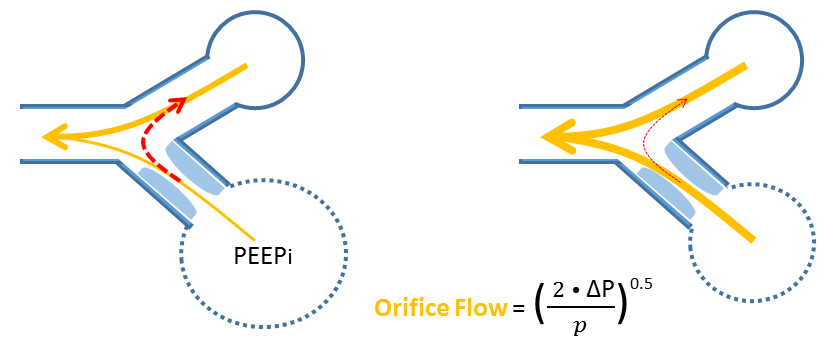
Figure 3: Orifice flow is inversely related to gas density (p); thus a low gas density will enhance expiratory flow. An obstructed lung unit [bottom left cartoon] will prolong the unit's time constant, delay emptying and lead to intrinsic PEEP [iPEEP]. Pendeluft [red dashed arrow] occurs at end-expiration from lung units of long to short time constants. Homogenous emptying in response to Heliox prevents this physiology [right cartoon].
Orifice flow is inversely related to gas density, such that expiratory flow through a narrowing will rise as gas density falls. This will diminish PEEPi and dynamic hyperinflation. Interestingly, this too has been found in the aforementioned studies [5-7]. To the extent that PEEPi is abolished, there will be diminished static breathing work as well. Indeed, Lee et al. reported that Ppeak, PEEPi and Pplat were all significantly reduced with the administration of Heliox [5]. The Heliox-associated reduction in PEEPi also improved cardiac output and diminished pulse pressure variation in their analysis!
Another consequence of PEEPi is that at end expiration, there can be continued airflow from lung units with prolonged time constants [bottom lung unit on the left of figure 3]. If some of this flow is directed to lung units without PEEPi [red dashed line] then air sloshes within the lung – so called ‘pendeluft’ physiology. This is wasted ventilation and effectively raises dead space. If lung units empty more homogenously, then the end-expiratory pendeluft phenomenon should also cease [8]. While Heliox is commonly found to diminish PEEPi and lower PaCO2, not all authors have found this to be due to homogenization of time constants [7].
Caveats, Concerns, Conclusion
Lowering gas density has salutary effects on both inspiratory and expiratory phases of the respiratory cycle. By reducing Ppeak, PEEPi and Pplat, dynamic and elastic work is reduced. Accordingly, the total mechanical power applied to the lung skeleton is diminished which may mitigate VILI. Lung units of differing time-constants have been found in ARDS [9], so this physiology may be germane beyond obstructive airways disease. The obvious drawback is that the density-dependent benefits of Heliox come at the expense of FiO2 and will limit application to severely hypoxemic patients. Accordingly, Heliox as an adjunct to extracorporeal oxygenation may hold clinical merit [10]. Regardless, as a lesson in applied physiology this thought experiment – I think – remains worthwhile; thanks Dr. C!
Please check out other posts in this series,
Cressoni, M., et al., Mechanical power and development of ventilator-induced lung injury. The Journal of the American Society of Anesthesiologists, 2016.
Hess, D.R., et al., The history and physics of heliox. Respir Care, 2006. 51(6): p. 608-612.
McGarvey, J.M. and C.V. Pollack, Heliox in airway management. Emergency medicine clinics of North America, 2008. 26(4): p. 905-920.
Gluck, E.H., D.J. Onorato, and R. Castriotta, Helium-oxygen mixtures in intubated patients with status asthmaticus and respiratory acidosis. Chest, 1990. 98(3): p. 693-698.
Lee, D.L., et al., Heliox improves hemodynamics in mechanically ventilated patients with chronic obstructive pulmonary disease with systolic pressure variations. Crit Care Med, 2005. 33(5): p. 968-973.
Tassaux, D., et al., Effects of helium-oxygen on intrinsic positive end-expiratory pressure in intubated and mechanically ventilated patients with severe chronic obstructive pulmonary disease. Crit Care Med, 2000. 28(8): p. 2721-2728.
Diehl, J.-L., et al., Helium in the adult critical care setting. Annals of intensive care, 2011. 1(1): p. 24.
Arnal, J., et al., Effect of helium–oxygen mixture on time constant inequalities in COPD patients during controlled ventilation. Critical Care, 2002. 6: p. 1-1.
Vieillard-Baron, A., et al., Pressure-volume curves in acute respiratory distress syndrome: clinical demonstration of the influence of expiratory flow limitation on the initial slope. Am J Respir Crit Care Med, 2002. 165(8): p. 1107-12.
Beurskens, C.J., et al., The potential of heliox as a therapy for acute respiratory distress syndrome in adults and children: a descriptive review. Respiration, 2015. 89(2): p. 166-174.