

ICU Physiology in 1,000 Words: ARDS - Part 1

Jon-Emile S. Kenny [@heart_lung]
“Often, as new knowledge progresses, old knowledge is abandoned or forgotten.”
-Luciano Gattinoni
In a succinct and current treatise, Gattinoni and Quintel outline the modern management of the acute respiratory distress syndrome [ARDS] [1]. It is imperative, they reason, that treatment of ARDS minimizes firstly, the mechanical power applied to the lungs and secondly, lung inhomogeneity.
The lung skeleton
The fibrous skeleton of the lung is composed of two fiber systems. Firstly, there is an axial system which is anchored to the hilum and arborizes along the airways towards the alveolar ducts [2]. Secondly, there is a peripheral system which is tethered to the visceral pleura and tracks inwardly towards the lung acini. These two aforementioned fiber systems associate at the alveoli and generate a continuous ‘lung skeleton’ [2]. Elastin and collagen are the major components of the lung skeleton and it is to this fibrous scaffold that the epithelial and endothelial cells of the lungs tether. When the skeleton of the lung is distended, there is an alteration of the lung parenchyma and accompanying cellular scaffolds. Excessive energy distributed to the skeleton may lead to a myriad of injuries, both indirectly via activation of mechanoreceptors but also by direct mechanical stress [2, 3].
Energy and work
Thus the energy applied to the lung’s fibrous skeleton may be the key determinant of ventilator induced lung injury [VILI]. As Gattinoni astutely notes, VILI is more precisely coined ventilation induced lung injury, as it may also be the consequence of spontaneous ventilation [4].
The total energy absorbed by the lung during a single breath is quantified by the joule; the joule is a measure of work. Consider that work is defined as a force required to move an object a given distance.
Because pressure is a force applied over a given area, and because volume is an area applied over a distance the following may be derived:
And, therefore:
Accordingly, upon the lung, work may be graphically depicted as the area bounded by the pressure-volume relationship [Figure 1A & B]. Further, there are two types of work applied to the lung during a breath – static and dynamic. Static work is the energy required to maintain volume while dynamic work is the requisite portion of energy driving gas flow and overcoming tissue resistance [e.g. tissues sliding over each other]. At the onset of a breath, a greater fraction of the work is dedicated to gas flow and tissue resistance [Figure 1B - blue shaded area]. As the breath continues a larger proportion of work is partitioned into maintaining lung volume [Figure 1B - red shaded area]. At the termination of the breath, all of the work is invested in the new volume; this is when flow – and therefore the fraction of dynamic energy – is zero. For more information on breathing work, please see chapter 1C and 1D.
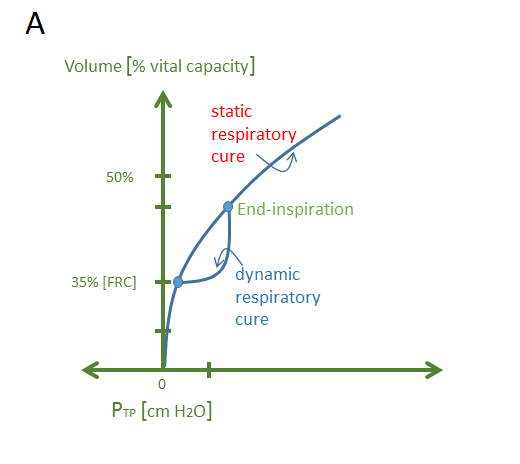
Figure 1A - Lung volume on y-axis and transpulmonary pressure [Ptp] on the x-axis. The Ptp, here, is defined as the proximal airway pressure less the pleural pressure [as estimated by the esophageal pressure]. FRC is the functional residual capacity
The summation of the static and dynamic work gives the total work for a single breath; however, when the total work is multiplied by the respiratory rate, the entire work per unit time is obtained and this is the mechanical power applied to the lung.
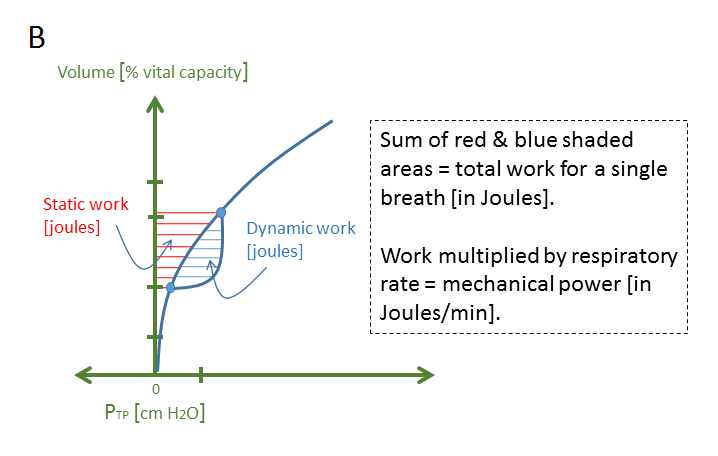
Figure 1B - as above, FRC = functional residual capacity, Ptp = transpulmonary pressure defined, here, as proximal airway pressure less the esophageal pressure.
Mechanical power
Since the publication of the landmark ARDSnet trial [5], the focus of VILI prevention – clinically – has been on minimizing lung volume and plateau pressure. As may be gleaned from the aforementioned diagram, these variables represent markers of the static work of a single breath. However, it has been found that respiratory rate, flow and even temperature are also co-mediators of VILI [6, 7]. Accordingly, the dynamic work applied to the lung also appears to facilitate some aspect of lung injury. To address these findings, Cressoni and colleagues have proposed a unifying hypothesis – mechanical power – which considers both static and dynamic energy applied to the lung over time [8].
In their porcine model, Cressoni and colleagues applied a tidal volume – known to be lethal – at varying respiratory rates. All other respiratory variables were maintained constant and all animals received paralytics. Consequently, mechanical power varied only by differences in respiratory rate and flow. The difference between the lowest and highest respiratory rate was 5-fold [3 breaths/minute versus 15 breaths per minute], yet the power increased 11-fold because flow is augmented with higher respiratory frequency. The power threshold for VILI occurrence was determined to be 12 Joules/minute. In confirmatory testing, a respiratory rate of 35 breaths per minute was selected for all animals, but at two different tidal volumes – one tidal volume which superseded the VILI threshold and one which did not. Again, only those ventilated at a mechanical power above 12 Joules/minute developed VILI. Mechanical power was also associated with final lung weight, increasing lung elastance, and diminished PaO2 to FiO2 ratio. Animals ventilated below this threshold, developed only isolated lung densities [8].
There may be clinical repercussions of this model should it extrapolate to the bedside. Firstly, peak pressure does indeed matter with respect to VILI as the peak pressure is a measure of dynamic work. Secondly, it raises theoretical concerns over the use of pressure-targeted modes of ventilation in ARDS as this method of ventilation prevents the clinician from completely controlling any of: lung volume, trans-pulmonary pressure or gas flow. Thirdly, mitigation of mechanical power may provide a mechanistic plausibility for the – albeit contentious – therapeutic effects of early paralysis in ARDS [9]; the absence of respiratory effort allows total control over lung volume, gas flow and minimizes trans-pulmonary pressure. Lastly, this model may explain the disappointing results of high-frequency oscillatory ventilation [10]; while tidal volume is extraordinarily reduced, the total mechanical power necessitated for lung oscillation may supersede the VILI threshold. Importantly, it should not escape the astute intensivist that the mechanical power applied to the lung’s fibrous skeleton may be cryptically high in other unconventional methods of mechanical ventilation, for example, airway pressure release ventilation [APRV].
Best,
References:
Gattinoni, L. and M. Quintel, How ARDS should be treated. Critical Care, 2016. 20(1): p. 1.
Gattinoni, L. and A. Pesenti, The concept of “baby lung”. Intensive Care Med, 2005. 31(6): p. 776-784.
Hotchkiss, J.R., et al., Pulmonary microvascular fracture in a patient with acute respiratory distress syndrome*. Crit Care Med, 2002. 30(10): p. 2368-2370.
Mascheroni, D., et al., Acute respiratory failure following pharmacologically induced hyperventilation: an experimental animal study. Intensive Care Med, 1988. 15(1): p. 8-14.
Laffey, J.G. and B.P. Kavanagh, Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury. N Engl J Med, 2000. 343(11): p. 812; author reply 813-4.
Suzuki, S., et al., Effect of core body temperature on ventilator-induced lung injury. Crit Care Med, 2004. 32(1): p. 144-149.
Rich, P.B., et al., Effect of rate and inspiratory flow on ventilator-induced lung injury. JOURNAL OF TRAUMA INJURY INFECTION AND CRITICAL CARE, 2000. 49(5): p. 903-911.
Cressoni, M., et al., Mechanical power and development of ventilator-induced lung injury. The Journal of the American Society of Anesthesiologists, 2016.
Papazian , L., et al., Neuromuscular Blockers in Early Acute Respiratory Distress Syndrome. New England Journal of Medicine, 2010. 363(12): p. 1107-1116.
Ferguson , N.D., et al., High-Frequency Oscillation in Early Acute Respiratory Distress Syndrome. New England Journal of Medicine, 2013. 368(9): p. 795-805.