

ICU Physiology in 1000 Words: High Flow Oxygen Therapy

Jon-Emile S. Kenny MD [@heart_lung]
That high flow oxygen applied via nasal cannula lends itself to treating hypoxemic respiratory failure may be obvious. With adequate heat and humidification, oxygen can be employed relatively comfortably at very high flow rates – upwards of 60 L/min – to the nares. At such rates, the effort of the patient is minimized and much less ambient air is entrained. Accordingly, precise fractions of inspired oxygen may be delivered up to 1.0. Further, the high flow of oxygen creates positive end-expiratory pressure [PEEP] and recruits end-expiratory lung volume [1, 2]. It is estimated that for every 10 L/min of oxygen flow applied that 0.7 cm of H2O of PEEP is generated with the mouth closed. If the mouth is open, this value falls to 0.35 cm H2O for each 10 L/min of flow [3]. The recruitment of lung with nasal high flow [NHF] oxygen undoubtedly contributes to improved PaO2/FiO2 ratios in patients with hypoxemic respiratory failure – even in obese post-operative patients who are at high risk for losing end-expiratory lung volume [1]. Additionally, in the relatively recent FLORALI trial, there was benefit suggested in patients with mild and moderate acute lung injury without hypercapnia as compared to non-invasive ventilation [4].
The Partial Pressure of Arterial Carbon Dioxide
Notably, patients with hypercapnia were specifically excluded from the FLORALI trial as non-invasive ventilation [NIV, e.g. BiPAP] has a strong evidence base for use in patients with hypercapneic respiratory failure [5]. Nevertheless, NHF does provide some assistance with arterial carbon dioxide tension, thus patients with hypercapnia and intolerance of NIV may derive some benefit from NHF. When considering the mechanistic details, it is important to refresh ourselves with the determinants of the partial pressure of arterial carbon dioxide [PaCO2].
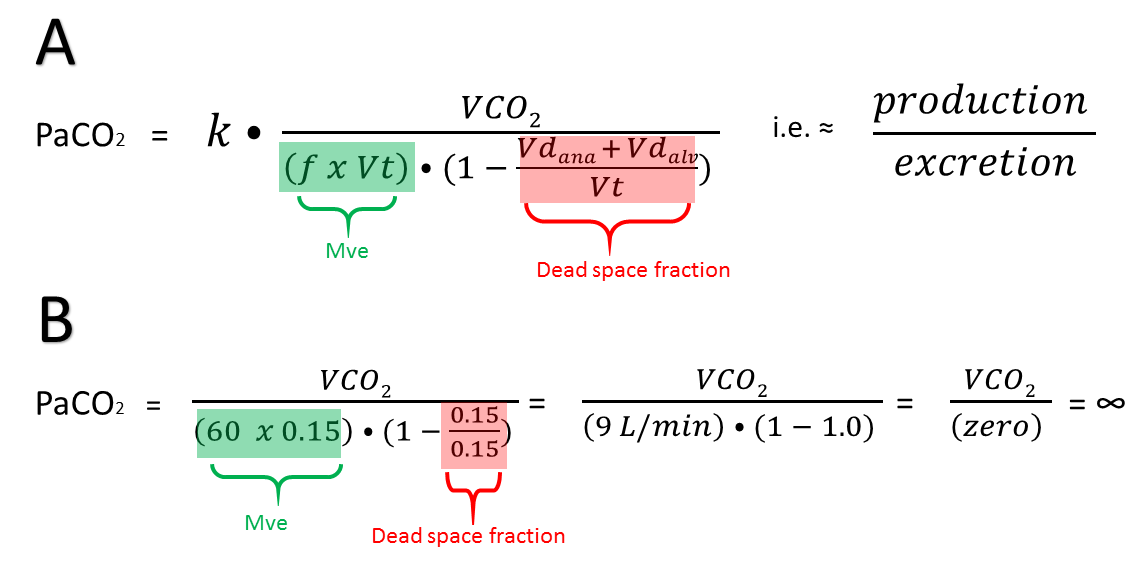
Figure 1: A. the determinants of PaCO2. B. The effect of rapid-shallow breathing is realized if one considers a patient breathing 60 breaths per minute with a tidal volume of 150 mL – the minute ventilation is 9 L/minute [60 x 0.150]. However, if we assume anatomic dead space to be roughly 150 mL, then the patient’s alveolar ventilation is zero! The patient is only washing gas in and out of his or her anatomical dead space; the dead space fraction is 100%! Carbon dioxide rises to infinity and death soon follows. Abrv: f is respiratory frequency, Vt is tidal volume, Vdana is anatomical dead space, Vdalv is alveolar dead space [together physiological dead space]. VCO2 is carbon dioxide production, Mve is minute ventilation.
As can be seen from the equation in 1A, the PaCO2 is directly related to tissue carbon dioxide production which makes intuitive sense. A patient with malignant hyperthermia, massive tissue oxygen consumption [VO2] and consequent supra-normal tissue carbon dioxide production [VCO2] will have a much higher PaCO2 unless it can be excreted by the lungs via alveolar ventilation.
Accordingly, alveolar ventilation is located in the denominator and is inversely-related to PaCO2 [6]. Alveolar ventilation is the fraction of the minute ventilation [Mve] that bathes the perfused alveoli. Thus, there is a portion of each inspiration which does not participate in gas exchange and this is known as ‘wasted ventilation’ or ‘dead space’ [6]. The dead space fraction is the total amount of dead space volume [Vd] out of each tidal volume [Vt]; that is, [Vd / Vt]. In turn, the normal dead space volume [Vd] is composed to two sub-types of dead space – anatomic dead space [Vd-ana] and alveolar dead space [Vd-alv]. Normally, the dead space volume Vd [also called physiological dead space] makes up 20-30% of each breath and this is almost entirely Vd-ana [7]. In other words, alveolar ventilation is 70-80% of the minute ventilation.
From the equation above, it should be clear that reducing PaCO2 may be enhanced by: reducing VCO2, increasing Mve [increasing respiratory rate or tidal volume] or reducing the dead space fraction [Vd/Vt].
Reducing dead space fraction is worth some elaboration, particularly in the setting of the commonly encountered patient with rapid-shallow breathing - see figure 1B. Note that the dead space fraction [Vd/Vt] necessarily rises as tidal volume [Vt] falls; consequently, any therapy which enhances deep tidal volumes will lower the dead space fraction and enhance carbon dioxide excretion [e.g. think Kussmauls’ respirations].
What may be less intuitive is that rapid breathing also raises Vd-alv [6]. Rapidly ventilating an alveolus/lung unit above and beyond its degree of perfusion [i.e. increasing V/Q ratio] also results in dead space, but this is not anatomical, it is alveolar. In summary, treating rapid breathing lowers alveolar dead space [Vd-alv], treating shallow breathing decreases dead space fraction [i.e. increases Vt, lowers Vd / Vt].
High Flow Nasal Cannula: work of breathing & alveolar ventilation
How might NHF lower the PaCO2? Probably by all of the aforementioned mechanisms. Firstly, patients in extremis can easily increase oxygen consumption VO2 – and therefore VCO2 – by 3-4 fold [8, 9]. In a recent study of patients with hypoxemic respiratory failure, NHF reduced the Ti/Ttot from 0.5 to 0.4 [10]. The Ti/Ttot is the ratio of inspiratory time to total breath cycle and is a surrogate for respiratory effort. A normal value is 0.33; values between 0.5 and 0.6 are considered unsustainable as fatigue and respiratory failure will set in [11]. In this study the pressure-time product also fell significantly with the application of NHF [10]; presumably, while VCO2 was not measured, it likely decreased via rest of the respiratory muscles.
NHF has other salutary effects on carbon dioxide balance. Nearly all investigations reveal that respiratory rate falls on NHF [2]; as above, this can reduce alveolar dead space [Vd-alv] by lowering ‘wasted ventilation’ [6]. Further, in healthy volunteers, Vt increased which lowered their dead space fraction [12]. Importantly, however, while asleep, the same volunteers on NHF had a reduction in Vt and, therefore Mve leading the authors to speculate that changes in minute ventilation on nasal high flow are sleep-wake dependent [12].
Not all investigations have shown an increase in tidal volume, but many show reductions in respiratory rate with stable or decreased PaCO2 – consistent with diminished VCO2 and/or increased efficiency of carbon dioxide excretion. An additional mechanism is the wash-out of nasopharyngeal dead space by high flow [13] which ameliorates Vd-ana. Importantly, the application of NIV via a tight-fitting face mask increases Vd-ana [1, 2]!
In summary, it is entirely possible that NHF effects all of the following: a reduction in VCO2, a reduction in Vd-ana, reduction in Vd-alv and, to the extent that tidal volume [Vt] increases, a potent fall in Vd/Vt.
Heliox Boost?
As described in this previous post, gas mixtures of helium and oxygen increase the fraction of laminar flow relative to turbulent flow and lower the resistance of the turbulent flow which remains. These effects increase airflow and therefore Vt for any given driving pressure and inspiratory time; as well, this will lower breathing work and, potentially, VCO2. To the extent that auto-PEEP falls and PEEP from nasal high flow stents open collapsed airways, diaphragmatic advantage will return and ventilation will be enhanced. Nevertheless, in the hypercapneic patient who is wholly intolerant or unable to cooperate with NIV, urgent endotracheal intubation should be considered before NHF plus heliox.
Please see more posts in this series,
References
Papazian, L., et al., Use of high-flow nasal cannula oxygenation in ICU adults: a narrative review. Intensive Care Med, 2016. 42(9): p. 1336-1349.
Nishimura, M., High-flow nasal cannula oxygen therapy in adults: physiological benefits, indication, clinical benefits, and adverse effects. Respir Care, 2016. 61(4): p. 529-541.
Parke, R.L., M.L. Eccleston, and S.P. McGuinness, The effects of flow on airway pressure during nasal high-flow oxygen therapy. Respir Care, 2011. 56(8): p. 1151-1155.
Frat, J.-P., et al., High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. New England Journal of Medicine, 2015. 372(23): p. 2185-2196.
Dwarakanath, A. and M.W. Elliott, Noninvasive ventilation in the management of acute hypercapnic respiratory failure. Breathe, 2013. 9(5): p. 338-348.
Kreit, J.W., Alterations in Gas Exchange Due to Low–Tidal Volume Ventilation. Annals of the American Thoracic Society, 2015. 12(2): p. 283-286.
Robertson, H.T., Dead space: the physiology of wasted ventilation. European Respiratory Journal, 2015. 45(6): p. 1704-1716.
Roussos, C. and P.T. Macklem, The respiratory muscles. N Engl J Med, 1982. 307(13): p. 786-97.
Macklem, P., Respiratory muscles: the vital pump. Chest, 1980. 78(5): p. 753-758.
Mauri, T., et al., Physiologic effects of high-flow nasal cannula in acute hypoxemic respiratory failure. Am J Respir Crit Care Med, 2017. 195(9): p. 1207-1215.
Banner, M.J., Respiratory muscle loading and the work of breathing. Journal of cardiothoracic and vascular anesthesia, 1995. 9(2): p. 192-204.
Mündel, T., et al., Mechanisms of nasal high flow on ventilation during wakefulness and sleep. J Appl Physiol, 2013. 114(8): p. 1058-1065.
Möller, W., et al., Nasal high flow clears anatomical dead space in upper airway models. J Appl Physiol, 2015. 118(12): p. 1525-1532.