

The Latest in Critical Care, 6/26/23 (Issue #6)

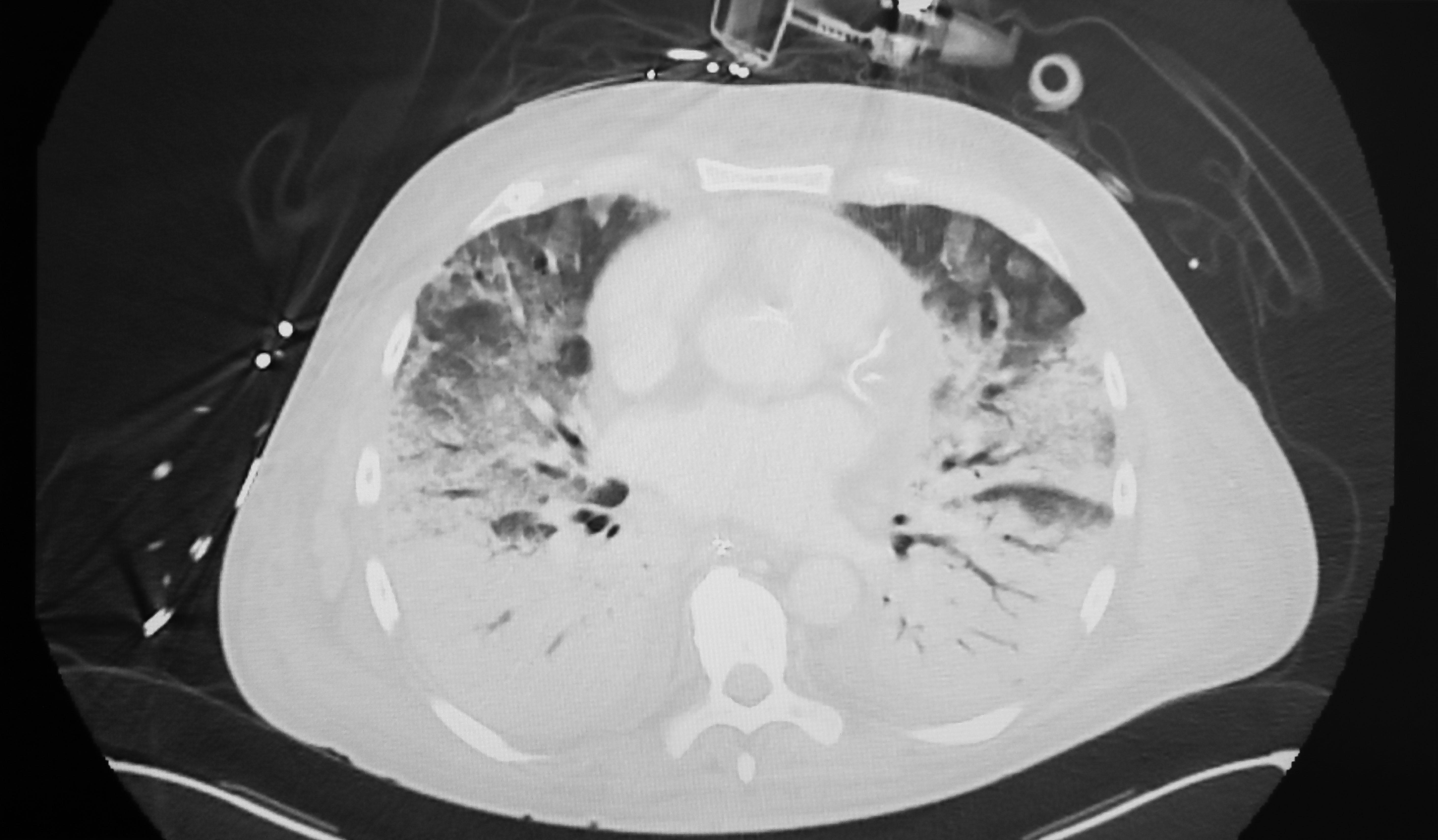
An expert panel broadened the definition of acute respiratory distress syndrome (ARDS).
They announced this at the American Thoracic Society meeting in May 2023. Thirty-two experts virtually to update the 2012 update (in Berlin), and declared that ARDS shall henceforth include anyone with:
PaO2/FiO2 ≤300 mmHg (on an arterial blood gas) or
SpO2/FiO2 ≤315m…
Keep reading with a 7-day free trial
Subscribe to PulmCCM to keep reading this post and get 7 days of free access to the full post archives.