

The Real-World Boards: Question #18
A 77-year-old man with shock, sepsis, tachycardia, and an abnormal heart rhythm

These are the Real-World Boards. As in the real world, there may be no single “right” answer, and you are only competing against yourself. Upgrade to the Lifelong Learner level for full access to all the questions and unlimited CME credits with an included Learner+ account.

You are working in the ED, where you “inherit” a boarding patient who arrived two shifts prior: a 77-year-old man with no known medical history who was brought to the ED with a fever of 38.4°C and confusion for two days. His white count was 18,000, with signs of infection on his urinalysis and hypotension unresponsive to fluids. He was treated with standardized sepsis care, including fluid resuscitation, antibiotics, and vasopressors. Cultures are pending. He was admitted to the ICU service, but does not yet have a bed.
You walk by his room and note the following rhythm on telemetry:
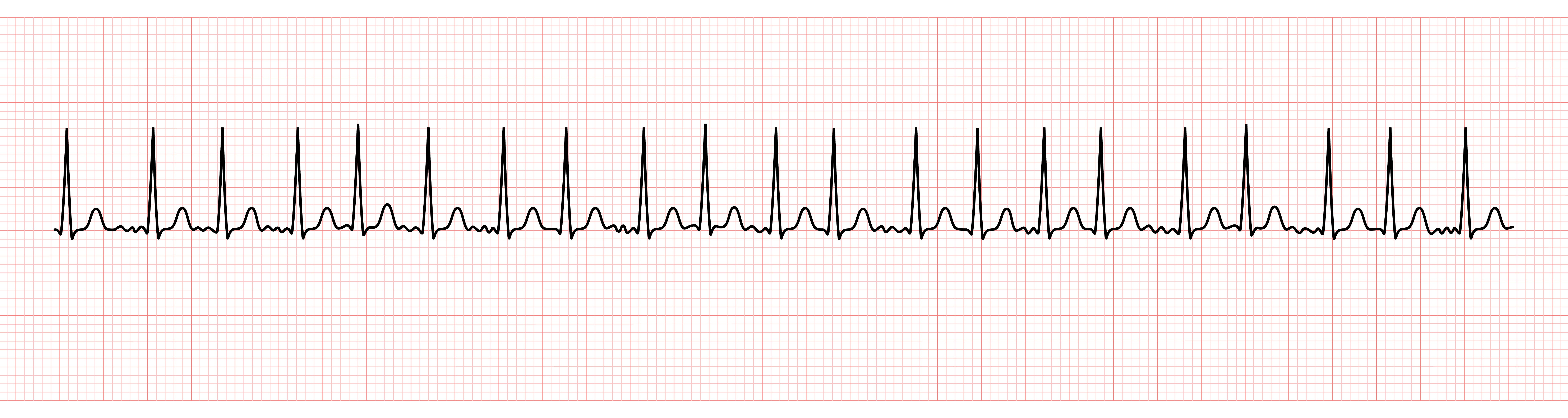
Blood pressure is 92/53, respirations 25, with SpO2 95% on 3L/min NC O2. He is mildly agitated; after calming down, the rate falls to ~140/min with a similar rhythm. He is confused and reasonably well-perfused distally.
You read the EMR. The intensivist’s note advises amiodarone infusion, but no order has been placed.
The cardiologist’s note specifically advises against using amiodarone, citing its risks. She advises AV nodal blocking agents, preferably diltiazem infusion or beta blockade. Again, no order was placed. Neither note mentions anticoagulation.

Atrial fibrillation (either new-onset or recurrent) is common in elderly patients with critical illness, especially sepsis: more than 20% of older adults with sepsis in ICUs develop atrial fibrillation with rapid ventricular response.
Both sepsis and atrial fibrillation can cause hypotension and tachycardia. In severe sepsis with atrial fibrillation with rapid ventricular response after appropriate volume resuscitation, it can be hard to ascertain the relative contributions to tachycardia and hypotension from the two coincident conditions. This uncertainty has direct implications for management decisions.