

The Real-World Boards: Question #30
The case of the questionably compromised interventionalist

These are the Real-World Boards. As in the real world, there may be no single “right” answer, and you are only competing against yourself. Upgrade to the Lifelong Learner level for full access to all the questions and unlimited CME credits with an included Learner+ account.
A 61-year-old man presented to the emergency department with worsening dyspnea over the past few days. He underwent a CT-angiogram, which diagnosed acute pulmonary embolism with right ventricular enlargement (RV/LV diameter = 1.2).
On presentation, his blood pressure, usually around 150/90, was 131/82, pulse 112, SpO2 94% on room air (usually 96-98%), and respirations 22 per minute. Troponin and pro-BNP were both elevated at >2x the upper limit of normal for each assay. Other than hypertension, obesity, and “prediabetes,” he has no recorded past medical history. He received enoxaparin 1 mg/kg of actual body weight.
You are a member of your center’s pulmonary embolism response team (PERT). After reviewing the relevant data, you arrive at the bedside to find the interventionalist’s physician assistant obtaining consent for an invasive procedure (either catheter-directed thrombolysis or mechanical thrombectomy; your center performs both).
You call the interventionalist, who doesn’t pick up, so you send a text.
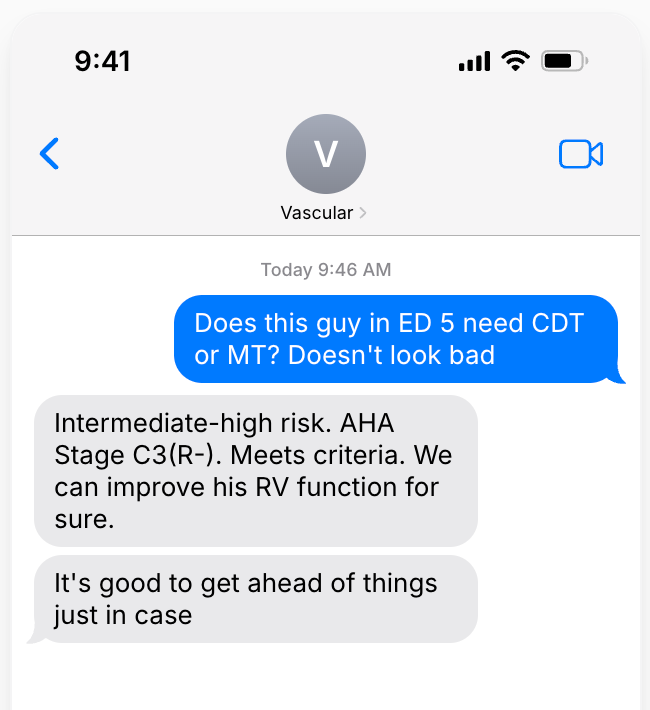
You find the patient’s condition to be roughly stable since arrival about an hour ago.
For their intuitively likely and anecdotally observed efficacy, catheter-directed thrombolysis and mechanical thrombectomy are increasingly being used to treat more severe acute pulmonary embolism in developed countries.
Because catheter-based therapies have not been meaningfully compared against the care standard of anticoagulation, though, their marginal benefits are unknown. Selecting which patients will be expected to benefit from invasive management (in excess of any procedural risks, which are also not well understood) often requires a leap of faith.