

The Real-World Boards: Question #39
Sepsis. Hypotension. Venous congestion.

These are the Real-World Boards. As in the real world, there may be no single “right” answer, and you are only competing against yourself. Upgrade to the Lifelong Learner level for full access to all the questions and unlimited CME credits with an included Learner+ account.
A 48-year-old man presents to the ED with worsening dyspnea, fever, and an increase in his chronic leg edema. He receives diagnoses of sepsis and decompensated heart failure, with suspected pneumonia based on nonspecific infiltrates on chest radiograph. His initial blood pressure is 100/70 with a normal heart rate. His SpO2 is 94% on 5 liters of nasal oxygen. Lactic acid is normal. Creatinine is 2.1 (baseline 1.5 mg/dL). Furosemide and ceftriaxone are provided.
Over the subsequent hours, his blood pressure falls to 85/45 (MAP 58) with pulse 110/min. His SpO2 is now 90% on high-flow nasal oxygen at FiO2 0.50, and respirations are 25 with increased work of breathing. ABG shows pH 7.35 / pCO2 33 / paO2 60.
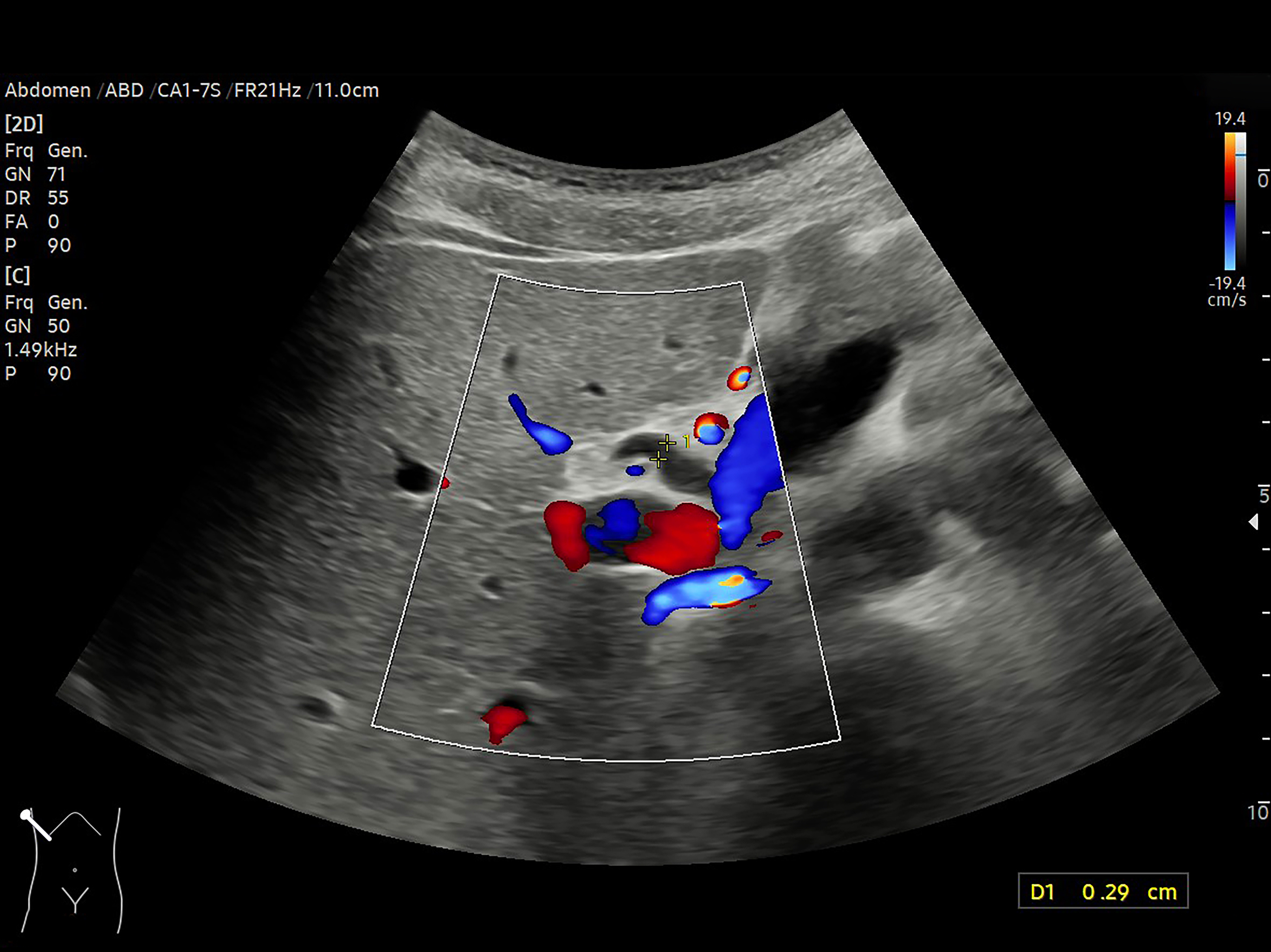
A bedside ultrasound shows a non-collapsing inferior vena cava during respirations. A passive leg raise is performed; two minutes later, his heart rate is 100/min (a 9% decrease). A jugular venous waveform is not well seen; you note a BMI of 40 and a thick neck.

Should patients with a diagnosis of septic shock (perhaps better termed sepsis-induced hypotension) first receive fluids, vasopressors, or both simultaneously? Few questions in critical care inspire as diverse and strongly held opinions as this.