

(UNLOCKED) The Real-World Boards: Question #33
A 57-year-old male with recent open-heart surgery suffers a cardiac arrest

These are the Real-World Boards. As in the real world, there may be no single “right” answer, and you are only competing against yourself. Upgrade to the Lifelong Learner level for full access to all the questions and unlimited CME credits with an included Learner+ account.
Please enjoy this next guest Real-World Boards question from Dr. Lloyd Tannenbaum, who authors the fantastic ECG Teaching Cases on Substack. —Ed.
You’re about halfway through your shift when a nurse comes to grab you. She tells you that Mr. Jackson in room 12 does not look well. She’d like you to come look at him.
As you walk to room 12, she briefs you on the patient: “Mr. Jackson is a 57-year-old male admitted to the ICU after a 4-vessel coronary artery bypass grafting. He is 72 hours out of surgery and had been doing well. He was making an uneventful recovery when he suddenly started to become very short of breath and complained of intense chest pain. He’s very pale and diaphoretic, so I asked one of the other nurses to stay in the room with him while I ran to go get you.”
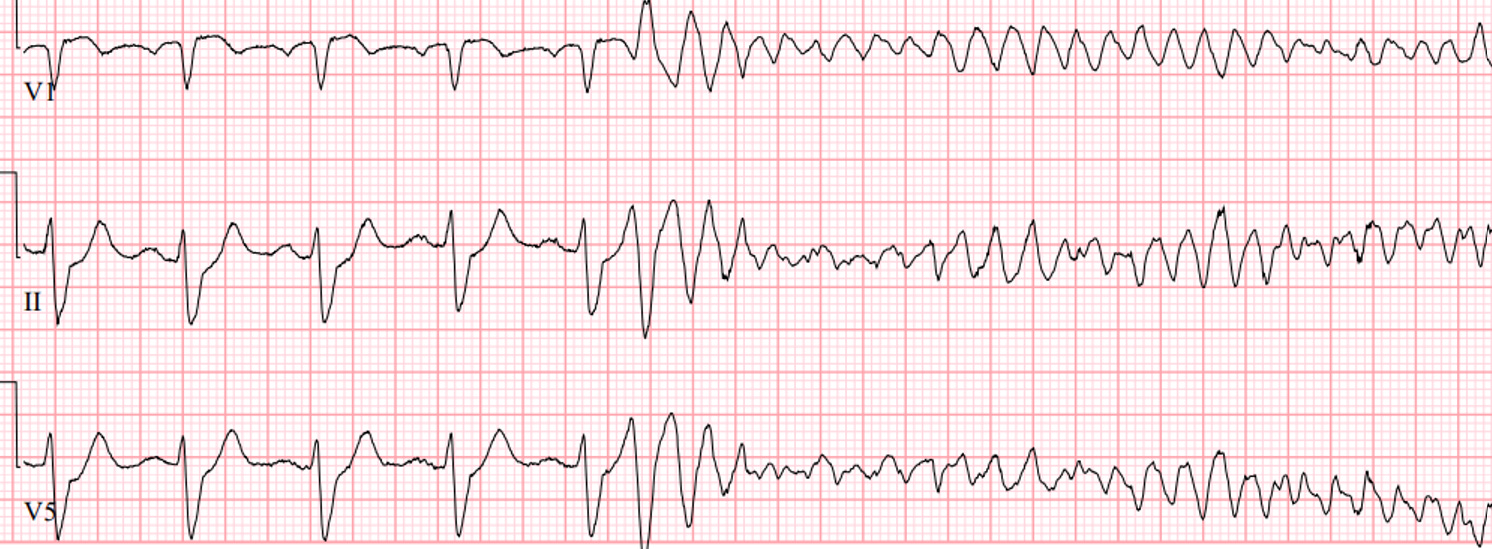
You walk into the room and see an unwell patient who is now unresponsive. Looking at the monitor, this is what you see. You’re unable to find a pulse.

Cardiac arrest after recent cardiac surgery tends to be witnessed, monitored, and due to discrete, rapidly reversible causes like tamponade, bleeding/hypovolemia, graft-related ischemia, or pacing failure, as compared to undifferentiated in-hospital arrests.
For these reasons, post-cardiac surgery patients in arrest are often best managed with a more flexible and situation-driven approach, not rigidly tethered to the standard advanced cardiac life support (ACLS) protocols.
Cardiac advanced life support, or CALS, was brought to international attention by Drs. Dunning et al in 2009 in their landmark paper, “Guidelines for resuscitation in cardiac arrest after cardiac surgery,” which proposed a set of suggested modifications to standardized society guidelines.
They advocated for specific resuscitation practices in patients in cardiac arrest up to 10 days after open-heart surgery. (Note: In the USA, CALS is also known as Cardiac Surgical Unit Advanced Life Support or CSU-ALS. For simplicity, we’ll just be referring to it here as CALS.)
In patients who arrest after recent open cardiac surgery, who are being managed in ICUs specialized in cardiac post-surgical care, the authors argued for deviating from the standard Advanced Cardiac Life Support (ACLS) algorithm in specific ways:
For ventricular fibrillation, asystole, or severe bradycardia, delay chest compressions until multiple attempts at defibrillation (in ventricular fibrillation) or pacing (in asystole or extreme bradycardia) have been performed.
Avoid epinephrine, which can cause unsafe increases in blood pressure.
Proceed to emergency re-sternotomy to definitively address potential causes for arrest (e.g., tamponade).
They argue for delaying chest compressions for defibrillation or pacing when reversible dysrhythmias are present:
In ventricular fibrillation, they advise three sequential defibrillation attempts, then starting chest compressions if cardiac arrest persists.
For asystole or pulseless bradycardia, they recommend pacing before starting chest compressions.
For non-bradycardic pulseless electrical activity, or if these measures fail, chest compressions should be performed.
This advice assumes defibrillation or pacing is immediately available and will not delay CPR.
While chest compressions (external cardiac massage) may be necessary initially, they recommend that emergency re-sternotomy (i.e., within five minutes) be considered.
Re-sternotomy provides for direct access to the heart, for internal cardiac massage (which is much more effective than CPR), as well as identification and management of potential causes for the arrest (e.g., tamponade or hemorrhage).
Although controversial when published in 2009, some version of the CALS framework has become standard in modern cardiac ICUs, and is formally or indirectly endorsed by major professional societies (including AHA, in the “Special Circumstances” section of its ACLS protocols).
AHA’s document advises spending no more than 1 minute shocking, pacing, or determining if the patient is in true PEA. Then, if necessary, start external CPR, recognizing that this may cause harm to the heart while compressing a split sternum, while the rest of the team prepares to re-open the chest.
One of the most interesting (and controversial) topics is not giving adrenalin (epinephrine or epi) to these patients if they arrest. This is mostly based on the data for giving epi in a code not being particularly strong, and a letter to the editor by Dr. Webb describing a situation where 1mg of epi was given in accordance with ACLS protocol when a post-op CABG patient arrested from a tension pneumothorax. Once a chest tube was placed, ROSC was rapidly achieved; however, a large amount of blood started coming out of his chest drains. When the patient had an emergent re-sternotomy, they found that the graft had burst open, likely secondary to the epi causing a huge spike in blood pressure. Dr. Webb encouraged the European Resuscitation Council to consider post-cardiac surgery patients a special population and recommend against giving epi if they arrest. That was followed by a formal 2017 guideline advising that “full doses of epinephrine should not be routinely given [during post-cardiac surgery arrests] owing to the danger of extreme hypertension if a reversible cause is rapidly resolved.”
Post-Cardiac Surgery Arrests: Different Etiologies, Different Approach
The major point that this paper makes and that these guidelines are based on, is that most causes of cardiac arrest in this patient population are reversible and related to their cardiac surgery. Getting back into the chest as quickly as possible (emergent re-sternotomy) leads to better outcomes.
In 2017, the Society of Thoracic Surgeons wrote an Expert Consensus for the Resuscitation of Patients who Arrest After Cardiac Surgery that re-examined these guidelines. They built on the initial flowsheet provided by the initial guidelines:
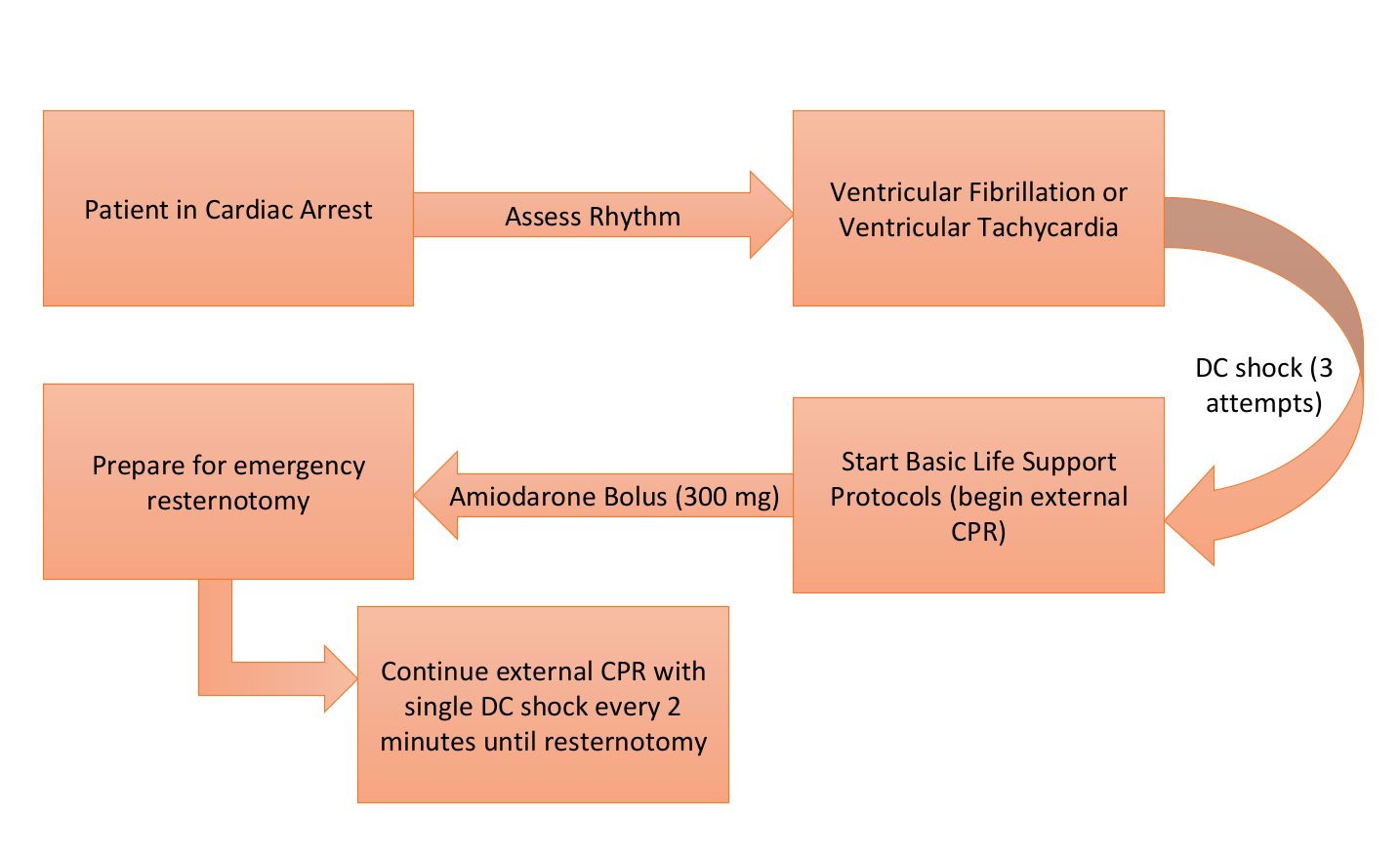
Walking through this figure, let’s start with early defibrillation (the orange arrow). Assuming that the team can get the machine set up to defibrillate under a minute, external CPR is not indicated before shocking 3 times back-to-back if the rhythm doesn’t convert. Why 3 shocks? Well, the authors pooled data from 15 papers and found that the chance of successfully cardioverting out of a dysrhythmia goes from 78% after the first shock to 35% after the second to 14% after the third. After 3 unsuccessful shocks, external CPR and emergent re-sternotomy are indicated, as your chances of converting out of a dysrhythmia by defibrillating after 3 failed attempts are extremely low.
Now take a look at the green and yellow arrows. If the patient is arresting and the rhythm isn’t amenable to defibrillation, consider pacing if the patient has severe bradycardia or asystole.
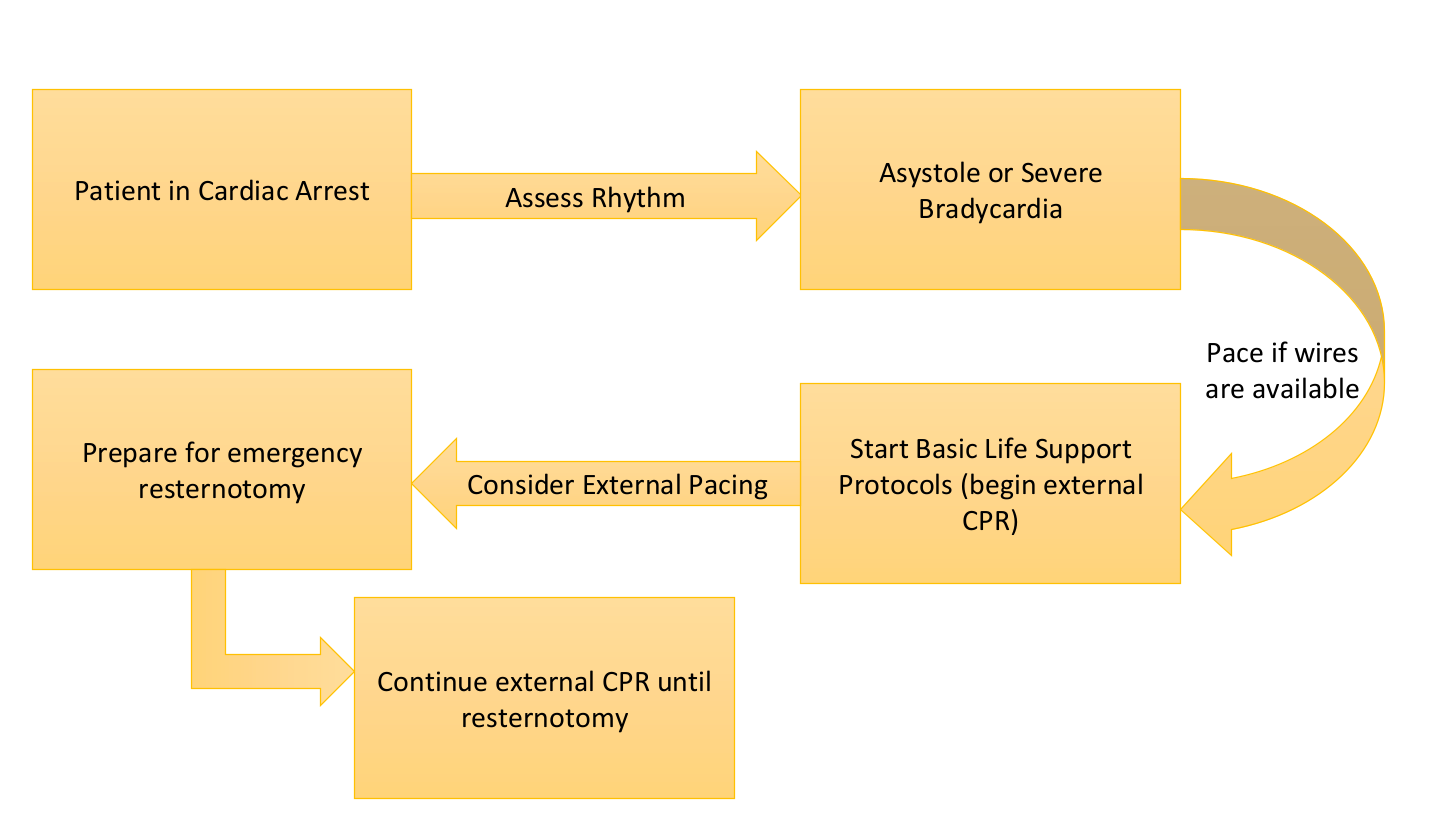
If the patient is in asystole or severe bradycardia (yellow arrow) and pacing wires are available, set the pacer to DDD mode between 80-100 beats per minute at max output and attempt pacing.
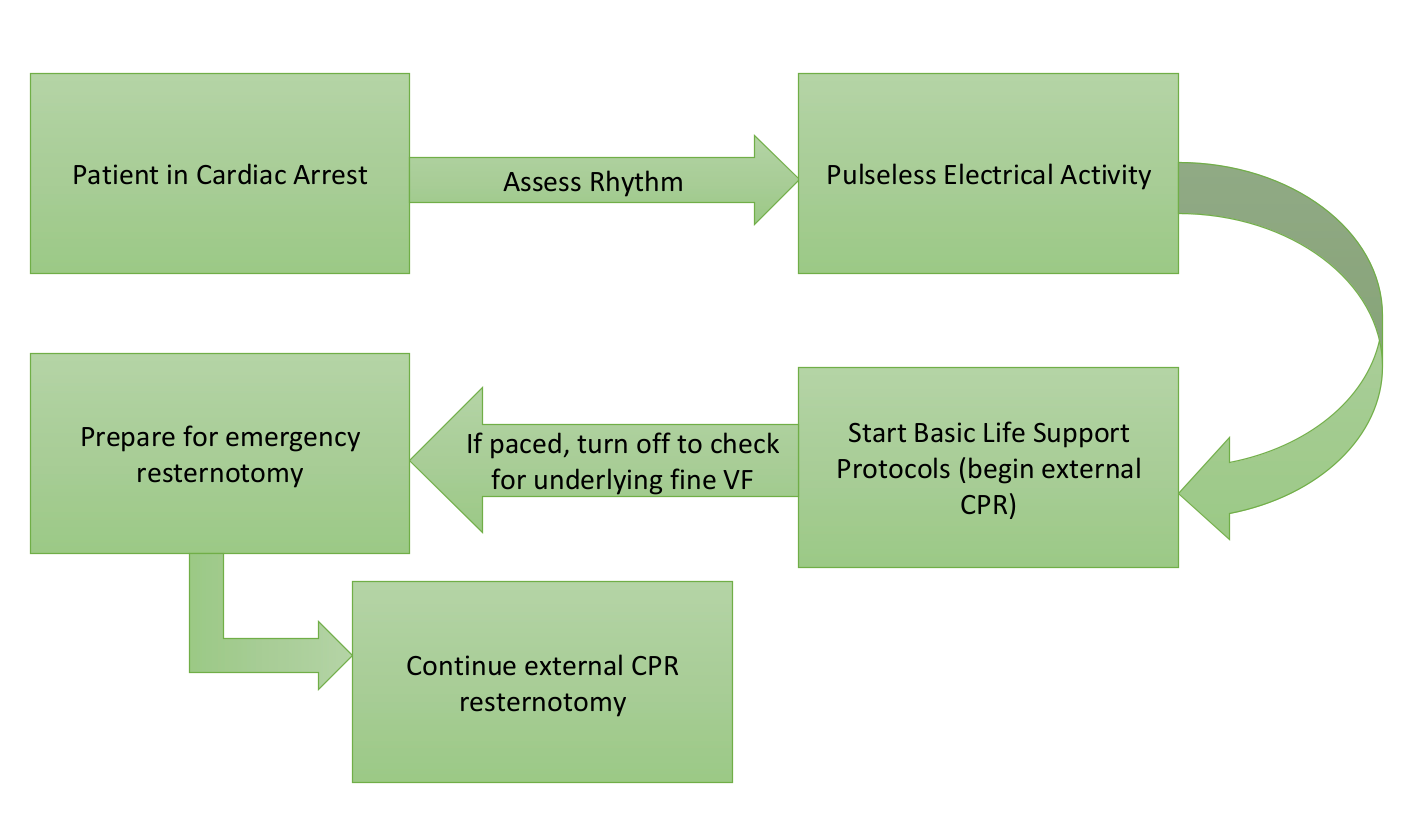
If the patient is in PEA (green arrow) and being paced, briefly turn off the pacemaker to evaluate for fine ventricular fibrillation, which may be masked by the pacer. If ventricular fibrillation is present, immediate defibrillation is indicated.
This paper also reexamined epinephrine in the peri-arrest state and arrest state. If the senior physician decides to use epi, push-dose epinephrine, which is a lower concentration (0.01mg/ml=10mcg/ml), is recommended. This is prepared by withdrawing 1 mL from the code epinephrine (1 mg/10 mL syringe) and diluting it with 9 mL of normal saline. The code leader will decide how much epi to give, but doses between 50 and 300 mcg are what the authors consider reasonable.
CALS Recap
Ventricular fibrillation: CALS recommends three rapid sequential defibrillation attempts (when immediately available) before initiating chest compressions. ACLS also endorses this in their “Special Circumstances” section.
Asystole or severe bradycardia: CALS prioritizes immediate pacing (if available) before external cardiac massage (chest compressions). ACLS endorses this as well.
Refractory arrest / true Pulseless Electrical Activity: CALS advocates chest compressions while preparing for emergency re-sternotomy to address reversible surgical causes. ACLS agrees.
Epinephrine: CALS does not recommend routine early epinephrine administration. When indicated, the standard ACLS code-dose concentration (1 mg/10 mL) should not be administered as a 1 mg bolus. Instead, push-dose epinephrine, which is a lower concentration, (0.01mg/ml=10mcg/ml) has been recommended. This is prepared by withdrawing 1 mL from the code epinephrine (1 mg/10 mL syringe) and diluting it with 9 mL of normal saline. ACLS does not comment on epinephrine for cardiac surgery patients. In any case, the senior physician running the code should be the one deciding if epi should or should not be given.
For more ECG Teaching Cases, please visit:

Reflect to earn CME with Learner+
Sample reflection: I reviewed and reflected on the clinical category of cardiac arrest occurring after recent cardiac surgery, and the deviation from standard resuscitation practices that may be indicated and beneficial in these special circumstances.

References
Part 10: Adult and Pediatric Special Circumstances of Resuscitation: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2025. Cao D, Arens AM, Chow SL, et al.
Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2020. Panchal AR, Bartos JA, Cabañas JG, et al.
The Society of Thoracic Surgeons Expert Consensus for the Resuscitation of Patients Who Arrest After Cardiac Surgery. The Annals of Thoracic Surgery. 2017.
2020 EACTS/ELSO/STS/AATS Expert Consensus on Post-Cardiotomy Extracorporeal Life Support in Adult Patients. The Journal of Thoracic and Cardiovascular Surgery. 2021. Lorusso R, Whitman G, Milojevic M, et al.
European Resuscitation Council Guidelines 2021: Cardiac Arrest in Special Circumstances. Resuscitation. 2021. Lott C, Truhlář A, Alfonzo A, et al.
Dunning J, Fabbri A, Kolh PH, Levine A, Lockowandt U, Mackay J, Pavie AJ, Strang T, Versteegh MI, Nashef SA; EACTS Clinical Guidelines Committee. Guideline for resuscitation in cardiac arrest after cardiac surgery. Eur J Cardiothorac Surg. 2009 Jul;36(1):3-28. doi: 10.1016/j.ejcts.2009.01.033. Epub 2009 Mar 17. PMID: 19297185.
Not quite in guidelines yet but we simultaneously start cannulating for Ecmo immediately. Results are pretty impressive. On average can be on Ecmo faster than a surgeon can be there to open chest, and then we can figure out what’s going on.
When you talk about pacing (if available), do you mean only if internal pacing available? Or also pacing with external pads?