

[UNLOCKED] The Real-World Boards: Question #40
Resistance is not always futile

These are the Real-World Boards. As in the real world, there may be no single “right” answer, and you are only competing against yourself. Upgrade to the Lifelong Learner level for full access to all the questions and unlimited CME credits with an included Learner+ account.

A 72-year-old man who resides in a nursing home is brought to the ED because of worsening lethargy and fevers. He has a history of recurrent urinary tract infections that is presumed due to prostatic hypertrophy, and was admitted with sepsis attributed to a UTI last month.
You review his urine culture data for the E. coli isolated on his admission last month:
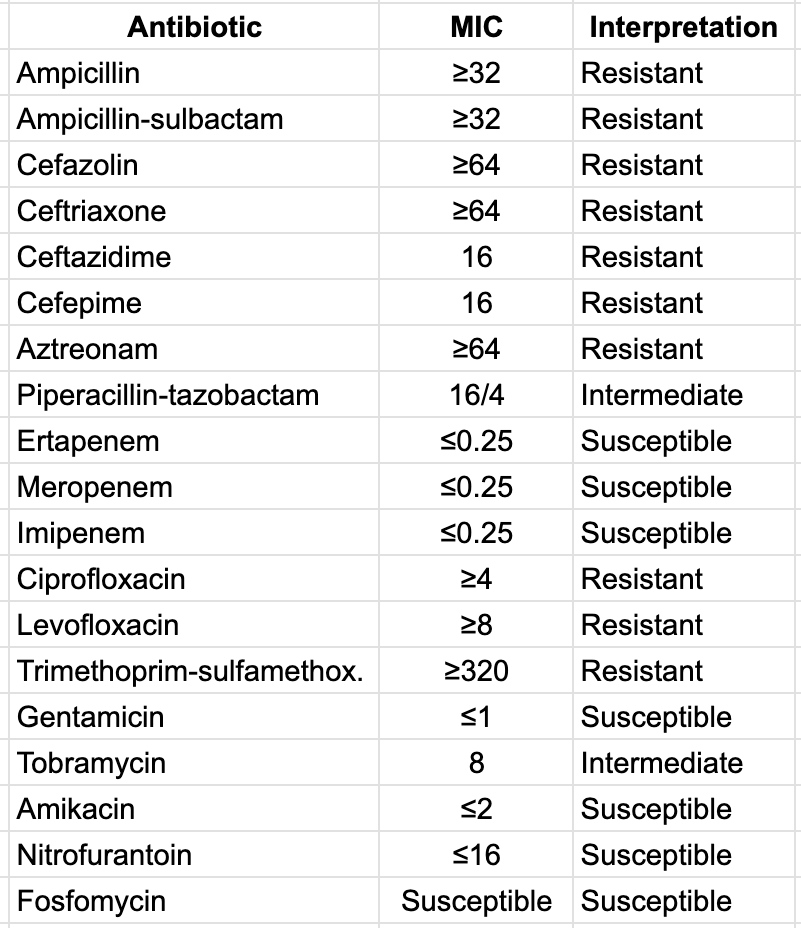
MRSA PCR screen from a nasal swab was negative at that time.
He is tachycardic, febrile, and has borderline hypotension. He is confused compared to his baseline. WBC is 20K, and creatinine is 2.9. In the ED, he is diagnosed with sepsis and provided a liter of I.V. crystalloid, piperacillin-tazobactam 3.5 g, and vancomycin 1.5 g I.V.
A CT of the abdomen shows no hydronephrosis or calculi.

Extended-spectrum beta-lactamase (ESBL) is an enzyme that can crack open the four-membered β-lactam ring, rendering the antibiotic ineffective.
ESBLs are encoded by genes located on large transferable modules (plasmids) that are easily shared between bacterial populations, most often Escherichia coli, Klebsiella pneumoniae, or Proteus mirabilis.
Infections by ESBL-producing gram-negative bacilli are notoriously lethal in the ICU, but as they tend to afflict the most vulnerable patients with longer ICU stays, more severe illness, and higher expected mortality, and also may often be present as colonizers alongside pathogenic bugs, their independent contribution to mortality is difficult to tease out precisely.
Generally speaking, urinary infections with ESBL-producing organisms are less often fatal than respiratory infections or primary bacteremias. Klebsiella is usually more virulent than E. coli. Septic shock with ESBL organisms has a higher mortality rate than with sensitive bacteria.
Microbiology labs may test for and report ESBL production, but it should be assumed anytime a gram-negative rod on the “usual suspects” list (E. coli, Klebsiella pneumoniae, Klebsiella oxytoca, and Proteus mirabilis) shows resistance to ceftriaxone (and often ceftazidime and aztreonam) but susceptibility to carbapenems.
Ceftriaxone resistance in Enterobacter cloacae, Klebsiella aerogenes, Citrobacter freundii, Serratia, etc., often suggests AmpC, not necessarily ESBL.
Narrower resistance (e.g., to ampicillin and/or cefazolin) does not imply ESBL, as many E. coli isolates are resistant to these agents.
Failure to adequately cover ESBL early is considered a likely major contributor to the excess mortality. As such, early appropriate antibiotic coverage for patients at risk is vital.
Meropenem is recommended for critically ill patients at high risk for ESBL organisms. Ertapenem is also effective, but does not cover Pseudomonas, which is often a concern in severe infections. Meropenem’s dose is reduced for renal impairment.
Although beta-lactamase inhibitors like tazobactam do thwart the ESBL enzyme in many patients, tazobactam has an unpredictable failure rate in ESBL-producing Enterobacteriaceae (aka Enterobacterales) in serious infections, especially bacteremia, sepsis, pneumonia, or ICU-level illness.
Gentamicin is considered an effective and appropriate agent against ESBL, but due to its risks for nephrotoxicity and ototoxicity, is considered second-line to meropenem for severe ICU-level infections.
Multiple newer β-lactam + β-lactamase inhibitor combination agents have entered the U.S. market in recent years. Ceftazidime-avibactam, meropenem-vaborbactam, imipenem-cilastatin-relebactam, ceftolozane-tazobactam, and cefiderocol all exhibit activity against ESBL organisms. These are generally reserved for carbapenem-resistant organisms to preserve their utility.
Oral nitrofurantoin or TMP-SMX may be a good option for uncomplicated ESBL UTIs, but are not recommended for severe infections. Fosfomycin is not recommended for K. pneumoniae or other organisms that may carry fosA genes, after a randomized trial found single-dose fosfomycin had more clinical failures than a 5-day course of nitrofurantoin.
Reflect to earn CME with Learner+
Sample reflection: I reviewed and reflected on infections due to known or suspected extended-spectrum beta-lactamase-producing gram-negative bacilli in the ICU, and the considerations for appropriate antimicrobial therapy.

References
Infectious Diseases Society of America 2023 Guidance on the Treatment of Antimicrobial Resistant Gram-Negative Infections. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2023. Tamma PD, Aitken SL, Bonomo RA, et al.
Infectious Diseases Society of America 2024 Guidance on the Treatment of Antimicrobial-Resistant Gram-Negative Infections. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2024. Tamma PD, Heil EL, Justo JA, et al.
Association Between Minimum Inhibitory Concentration, Beta-Lactamase Genes and Mortality for Patients Treated With Piperacillin/Tazobactam or Meropenem From the MERINO Study. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2021. Henderson A, Paterson DL, Chatfield MD, et al.
Ceftolozane-Tazobactam Versus Meropenem for Definitive Treatment of Bloodstream Infection Due to Extended-Spectrum Beta-Lactamase (ESBL) and AmpC-producing Enterobacterales (”MERINO-3”): Study Protocol for a Multicentre, Open-Label Randomised Non-Inferiority Trial. Trials. 2021. Stewart AG, Harris PNA, Chatfield MD, Littleford R, Paterson DL.
Multidrug-Resistant Gram-Negative Bacterial Infections. Lancet. 2025. Macesic N, Uhlemann AC, Peleg AY.
Extended-Spectrum Β-Lactamase-Producing Enterobacteriaceae: Update on Molecular Epidemiology and Treatment Options. Drugs. 2019. Peirano G, Pitout JDD.
Carbapenem Use in Extended-Spectrum Cephalosporin-Resistant Enterobacterales Infections in US Hospitals and Influence of IDSA Guidance: A Retrospective Cohort Study. The Lancet. Infectious Diseases. 2024. Walker MK, Diao G, Warner S, et al.
Preserving the Antimicrobial Arsenal: Exploring Alternatives to Carbapenems in ESBL Battles Within the Southeast of Ireland. Journal of Medical Microbiology. 2025. Ali S, Tobin A, Lapthorne S, et al.