

ICU Physiology in 1000 Words: Airway Pressure Release Ventilation – Part 1

Jon-Emile S. Kenny MD [@heart_lung]
While the lung in the throes of acute respiratory distress syndrome [ARDS] is shrunken, edematous and inflamed, a basic management maneuver is to ‘recruit’ lost pulmonary surface area. In other words, unfold alveolar-capillary units with the ventilator like a respirothoracic party horn. One ‘unconventional’ method of maximizing and maintaining lung volume is airway pressure release ventilation [APRV].
Imagine applying 30 cm H2O of continuous positive airway pressure [CPAP] to a spontaneously breathing patient; then every 5 seconds or so, the airway pressure is released from 30 to atmospheric pressure [0 cm H2O] for ~ 0.5 seconds. Following this momentary release, the 30 cm of H2O is rapidly re-applied. Importantly, the patient breathes on his or her own throughout; this is, essentially, APRV.
Yet this facile description belies the complicated literature surrounding APRV, largely for the same reason that mechanical ventilation, in general, drives new trainees bonkers – erratic clinical application and nomenclature between different ventilators, institutions and investigations [1, 2]. What was called APRV in the late 1980s is quite different from its application today; what is called APRV on one ventilator today may be called something quite different on another contemporary ventilator [e.g. BiLevel, BiVent, BiPhasic and DuoPAP] [3].
For the above stated reasons, this post will make a key distinction between 2 broad APRV ‘types’ originally coined by Habashi in 2005 [1, 4]. First, APRV approaches that ‘fix’ settings will be termed F-APRV while those approaches that personalize APRV settings based on respiratory mechanics between patients and within one patient across the arc of an illness will be designated P-APRV.
Fixed or Personalized?
The 4 main settings of APRV establish the duration and degree of its 2 different pressure sets. That is, the value of the high pressure [P-High] and the time spent at said high pressure [T-High]. Similarly the clinician selects the value and duration of the lower pressure [P-low and T-low, respectively]. These settings may invite the clinician to recon APRV as a type of BiPAP – just with longer inspiratory time – however, the change in applied airway pressure is not – save for very uncommon varieties – triggered by the patient. APRV applies inverse-ratio, pressure-limited, time-cycled breath-types and allows the patient to breathe spontaneously throughout [5].
Ironically, fixed forms of APRV [F-APRV] can be quite variable. Generally, F-APRV encompasses settings that include a relatively long T-low. Indeed, the duration of the T-Low may be so prolonged that the waveform appears similar to BiPAP [6]. Accordingly, F-APRV, as defined by Habashi, will encompass settings that include relatively short T-High [i.e. less than 90% of the entire cycle time] and maintain a T-Low that is invariant in the face of changing respiratory mechanics. P-APRV, by contrast, is defined by: a T-High that is at least 90% of the total cycle time, T-Low titrated to changing respiratory mechanics and P-Low that is set to zero [1] [see figure 1].
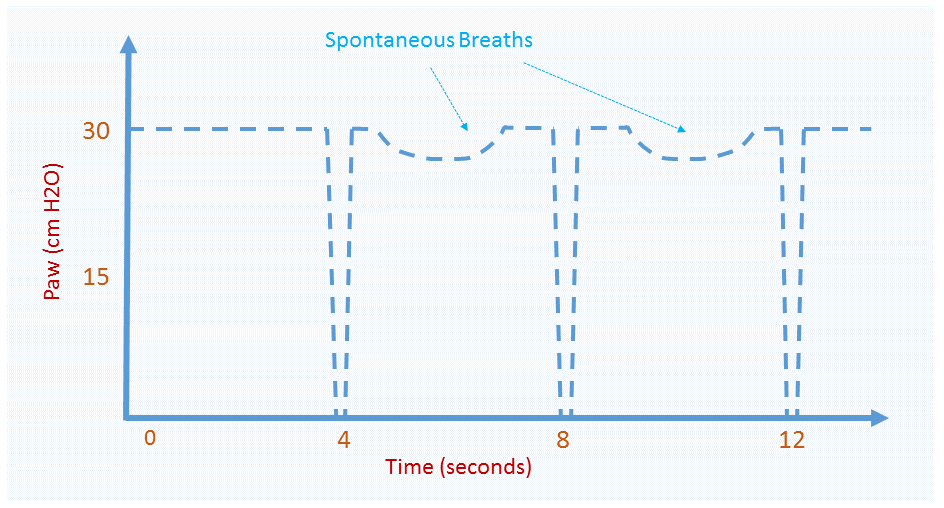
Figure 1A: example of P-APRV with P-High of 30 cm H2O and P-Low of zero H2O. T-High is about 4 seconds and T-Low is very short. How T-Low is set in P-APRV is described in part 2. Spontaneous breaths are seen as downward deflections in the airway pressure on y-axis.
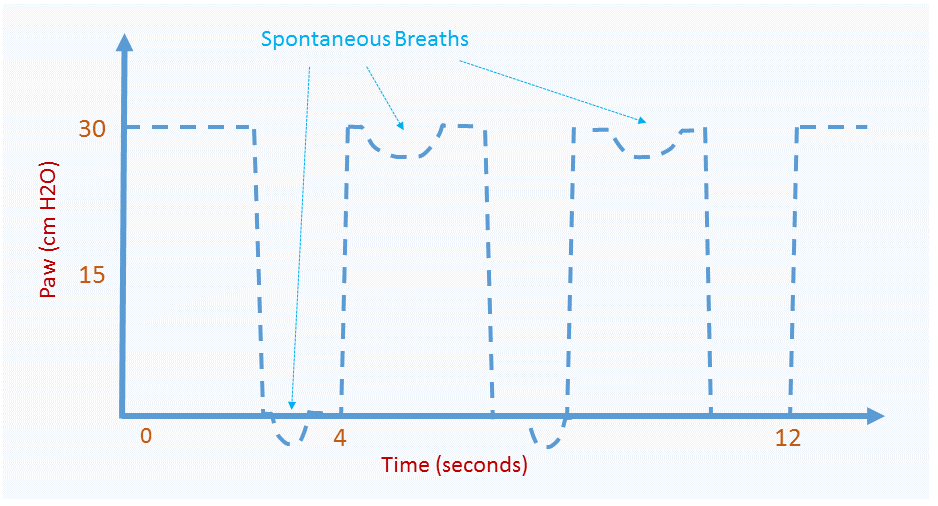
Figure 1B: Example of F-APRV with P-High at 30 cm H2O and P-Low at zero cm H2O but T-High and T-Low are now almost equal. With longer T-Low, spontaneous breaths can be seen at P-Low
T-Low & Time Constants
A key aspect of P-APRV is that the duration of time at P-Low is very short. How short? This depends upon the respiratory mechanics of the patient. As the ultimate goal of APRV is to ‘open the lung and keep it open’, and release duration [i.e. T-Low] varies inversely with expiratory lung volume [EELV], then a short T-Low is desired. In other words, a brief T-Low generates large EELV and vice versa. Intuitively, a long T-low will allow more time for lung volume to empty while a short T-low will prevent lung empty – resulting in auto-PEEP.
Accordingly, one reasonable criticism of APRV is that it generates ‘hidden PEEP’ – and it does. Certainly hidden PEEP raises the strain on the lung [i.e. the change in lung volume relative to its resting volume] and the stress [i.e. the pressure across the lung tissue] [7]. Can a clinician titrate just how much stress and strain is generated by changing T-Low? This is an important question given that excessive strain and stress are the mediators of volutrauma and barotrauma, respectively [8].
One mathematical approach is to assume that lung emptying acts as a single compartment composed of a resistance [e.g. airway] and compliance [e.g. alveolus] in series [9]. In this simplified system, change in respiratory characteristics follow a mono-exponential decay with respect to time [see figure 2].
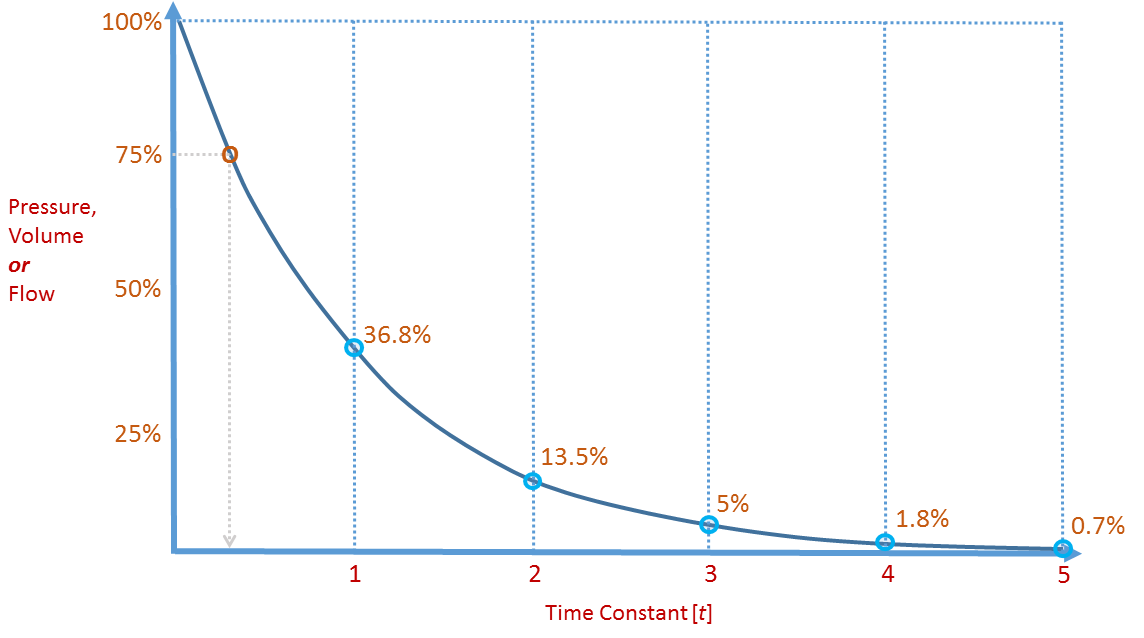
Figure 2: See text for details - the grey line at 75% will become important in part 2 when discussing how T-Low is set in P-APRV
The time it takes for pressure, volume or flow to fall by 63% of its value is termed the time constant [t] and can be estimated for the respiratory system as the product of respiratory system compliance [Crs] and resistance [Rrs] [3]. For example, if an ARDS patient has a Crs of 30 mL/H2O and a total Rrs of 15 cmH2O/L/s [10], then t is 0.030 L/H2O x 15 cmH2O/L/s [note mL to L change for compliance] = 0.45 seconds. Accordingly, airway pressure is expected to decay by 63% following 0.45 seconds of expiration. If the initial airway pressure were 30 cm H2O, then following 0.45 seconds of expiration, the airway pressure is expected to fall by 19 cm H2O to 11 cm of H2O. Following another time constant, airway pressure would drop by another 63% [i.e. from 11 to 4 cm H2O]. Implicit in these calculations is that the P-Low is set to atmospheric pressure [0 cm H2O] which maximizes expiratory pressure and volume drop and therefore carbon dioxide excretion. Indeed, P-Low of zero is inherent to the P-APRV definition [1].
Problems with Time Constants
There are a few problems with using t to predict auto-PEEP during P-APRV. The first is that the lung is not a simple ‘tube and bag’ model upon which mono-exponential decay is based [9]. The lung contains many units in parallel of differing resistance and compliance. As well, resistance and compliance are tethered physiologically. For example, airway caliber depends upon lung volume – with higher lung volumes tethering open peripheral airways. Complicating matters, the compliance of the respiratory system also changes with volume. Additionally, calculated resistance is affected by compliance because the stiffness of the lungs partly determines flow, independent of airway caliber. Only when all time constants are equal is total resistance independent of compliance [11]. Uniform t is unlikely in the diseased ARDS lung with multiple abnormal lung compartments in parallel. Indeed, this has been demonstrated in multiple studies of total airway resistance in ARDS [11-14]. Further, both resistance and compliance are dynamic throughout the course of ARDS and its treatment. Thus, resistance and compliance would have to be repeatedly measured to adjust T-Low which would be clinically burdensome. Finally, because different ventilators handle air-trapping differently, there can be substantial variation in the amount of auto-PEEP after 1 time constant solely as a function of the type of ventilator used [15]!
In the following part, a means to circumvent time constants to adjust T-Low is described.
Please check out other posts in the ‘1000 Word’ series,
JE
Dr. Kenny is the cofounder and Chief Medical Officer of Flosonics Medical; he is also the creator and author of a free hemodynamic curriculum at heart-lung.org
References
Jain, S.V., et al., The 30-year evolution of airway pressure release ventilation (APRV). Intensive care medicine experimental, 2016. 4(1): p. 11.
Henzler, D., What on earth is APRV? Critical Care, 2011. 15(1): p. 115.
Daoud, E.G., H.L. Farag, and R.L. Chatburn, Airway pressure release ventilation: what do we know? Respiratory care, 2012. 57(2): p. 282-292.
Habashi, N.M., Other approaches to open-lung ventilation: airway pressure release ventilation. Critical care medicine, 2005. 33(3): p. S228-S240.
Mireles-Cabodevila, E. and R.M. Kacmarek, Should airway pressure release ventilation be the primary mode in ARDS? Respiratory care, 2016. 61(6): p. 761-773.
Davis, K., et al., Airway pressure release ventilation. Archives of Surgery, 1993. 128(12): p. 1348-1352.
Gattinoni, L. and A. Pesenti, The concept of “baby lung”. Intensive care medicine, 2005. 31(6): p. 776-784.
Gattinoni, L., et al., The" baby lung" became an adult. Intensive care medicine, 2016. 42(5): p. 663-673.
Melo e Silva, C.s.A. and C.E.G.d.S. Ventura, A simple model illustrating the respiratory system’s time constant concept. Advances in physiology education, 2006. 30(3): p. 129-130.
KOUTSOUKOU, A., et al., Expiratory flow limitation and intrinsic positive end-expiratory pressure at zero positive end-expiratory pressure in patients with adult respiratory distress syndrome. American journal of respiratory and critical care medicine, 2000. 161(5): p. 1590-1596.
Bates, J., A. Rossi, and J. Milic-Emili, Analysis of the behavior of the respiratory system with constant inspiratory flow. Journal of Applied Physiology, 1985. 58(6): p. 1840-1848.
Pelosi, P., et al., Alterations of lung and chest wall mechanics in patients with acute lung injury: effects of positive end-expiratory pressure. American journal of respiratory and critical care medicine, 1995. 152(2): p. 531-537.
Vieillard-Baron, A., et al., Pressure–volume curves in acute respiratory distress syndrome: clinical demonstration of the influence of expiratory flow limitation on the initial slope. American journal of respiratory and critical care medicine, 2002. 165(8): p. 1107-1112.
Al-Rawas, N., et al., Expiratory time constant for determinations of plateau pressure, respiratory system compliance, and total resistance. Critical Care, 2013. 17(1): p. R23.
Daoud, E.G. and R.L. Chatburn, Comparing surrogates of oxygenation and ventilation between airway pressure release ventilation and biphasic airway pressure in a mechanical model of adult respiratory distress syndrome. Respiratory investigation, 2014. 52(4): p. 236-241.