

ICU Physiology in 1,000 Words: ARDS - Part 2

Jon-Emile S. Kenny [@heart_lung]
Gattinoni and Quintel have, very recently, outlined their approach to managing the acute respiratory distress syndrome [ARDS] [1]. They argue that treatment of ARDS should minimize firstly, the mechanical power applied to the lungs – as described in part 1. Secondly, Gattinoni and Quintel note that, in the treatment of ARDS, lung inhomogeneity should be mitigated – using optimal positive end-expiratory pressure [PEEP] and the prone position; these topics will be the focus herein.
Strain and stress
The volume applied to the lung is the strain placed upon the lung skeleton, described previously. Importantly, the strain is not simply the absolute volume administered by the ventilator, but rather it is the volume applied by the ventilator relative to the volume within the lung available for gas exchange [2]. In progressively severe ARDS, the volume within the lung accessible for ventilation becomes increasingly small. This cryptic lung volume was first appreciated when ARDS was initially studied with CT scans in the 1980s and gave rise to the notion of the ‘baby lung’ [2]. Consider two 70 kg patients, one with a ‘baby lung’ size of 200 mL versus the other with a baby lung size of 800 mL. The application of a 400 mL breath to each of these fictitious patients will result in a very different strain, and consequently different stresses to the lung skeleton.
Stress refers to the fiber tension within the lung skeleton, that is, primarily the tensile properties of collagen. In other words, in response to a given strain, there is an internal tension – a molecular rearrangement – generated within the fibrous lung skeleton and this is stress [2, 3]. Clinically, stress is approximated by the trans-pulmonary pressure or the airway pressure less the pleural pressure. Stress and strain are related by a constant which is specific to the tensile properties of the deformed material. This constant is called the specific elastance and, interestingly, even within severe ARDS the specific elastance of the lung is normal [2, 4]. Simply, the enlarged strain and stress of the lung arises not because the diseased lung is stiff, but rather small [2]. The relationship between stress, strain and elastance is completely analogous to the relationship between pressure, volume and compliance.
Lung inhomogeneity and stress raisers
Appreciation of strain and stress within the context of pulmonary mechanics is important when considering the ‘stress raiser’ hypothesis. Initially proposed by Mead et al. over 40 years ago, the 'stress raiser' theory considers that local stress is multiplied when a given stress or strain is directed towards inhomogeneous material [5]. Consider figure 1 below. It can be seen that the inhomogeneous portion of the lung [i.e. in 1B] acts as a ‘stress raiser’ locally on its neighboring lung units. An equivalent volume is applied to both lung unit A and B, however, the portions of lung around the ‘stress raiser’ experience a much greater regional stress.
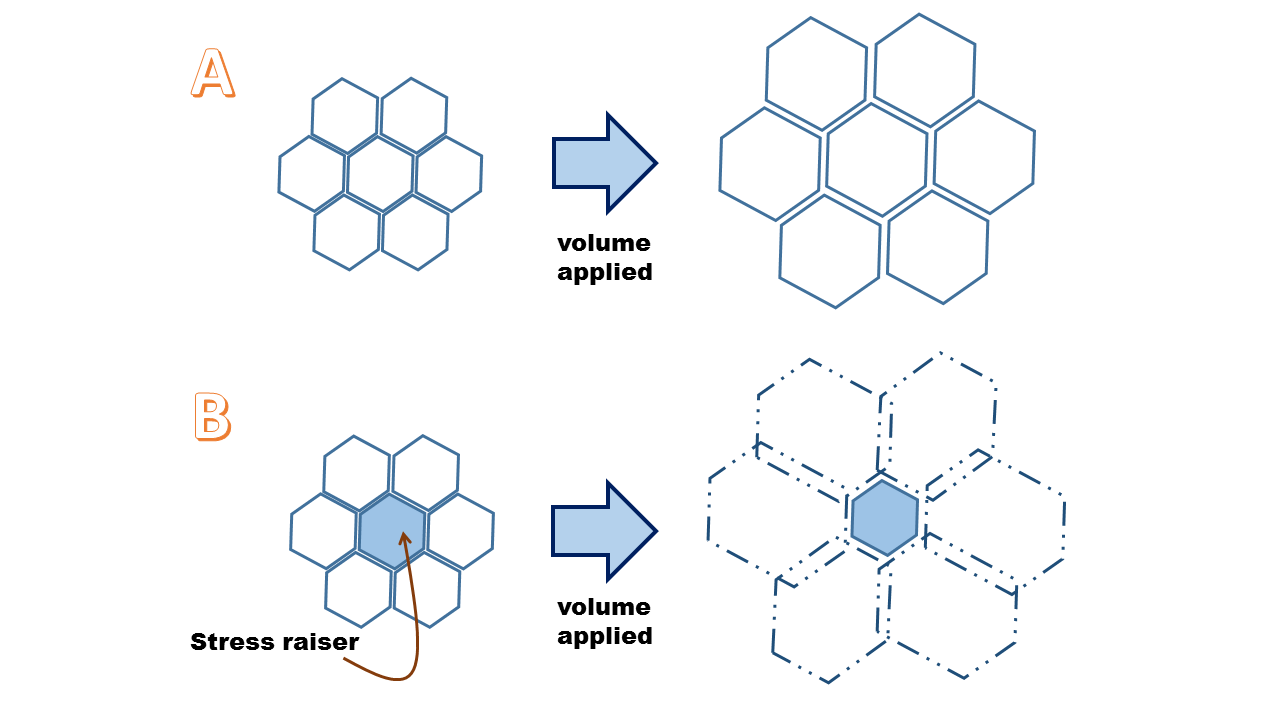
Figure 1: Example A represents the application of volume to a normal lung unit. Example B demonstrates a 'stress raiser' whereby the same volume is applied as in A, yet the portion of lung surrounding the stress raiser carries an increased stress and strain.
In a porcine model, Cressoni and colleagues found that in normal lungs, ventilator-induced lung injury [VILI] began around areas of the lung that are anatomically inhomogeneous [e.g. at the pleural/alveolar interface, blood vessels and airways] lending credence to the ‘stress raiser’ hypothesis [6]. Importantly, any structural anomaly may be a stress raiser [e.g. atelectasis, age-related anatomical changes, scar, edema, secretions, consolidation, etc.]
PEEP
PEEP is perhaps the easiest means by which lung inhomogeneity – and therefore the degree of ‘stress raisers’ – can be attenuated [7, 8]. Using a unique, voxel analysis of CT scans of human subjects, Cressoni and colleagues assessed lung inhomogeneity in ARDS and also in response to increased airway pressure [8]. They found that the scope of lung homogeneity was associated with ARDS severity, dead space fraction and patient outcome. Additionally, they found that augmentation of PEEP diminished lung inhomogeneity, in totality. Importantly, however, in the individual patient, PEEP can have varied effects on lung inhomogeneity – that is augment, diminish or unalter it. Two means by which the effect of PEEP on thoracic mechanics can be quantitatively or qualitatively judged are the driving pressure and stress index, respectively. At the optimum level, PEEP prevents intertidal collapse and maintains recruited lung open [9, 10] – both means of reducing 'stress raisers.'
Prone position
Trans-pulmonary pressure, or stress – described above – is not uniform within the normal lung. Because of both gravitational forces and the adaptation of the lung and chest wall to match each other’s shape, alveolar stress tends to be greatest at the ventral portion of the lung, when supine [11]. When placed in the prone position, gravitational effects tend to compress the ventral portions of the lung, but the adaptation of the lung to the chest wall shape resists the compressive gravitational force [11]. Consequently, the alveolar stress from the dorsal to the ventral regions is more homogeneous in prone. Perfusion of the lungs tends to be similar between the supine and prone positions; accordingly, ventilation-to-perfusion ratios are more consistent while prone [12].
In severe ARDS, there can be increased edema and lung injury throughout, resulting in a ubiquitously elevated hydrostatic pressure within the lung. This, ‘superimposed pressure’ may be 4-5 time normal and results in compression of the dorsal lung [11]. The dependent lung is then degassed giving the impression of dependent opacities. Bone [13] coined this ‘sponge lung’ to illustrate a boggy mass squeezed under its own weight. Empirically, flipping a patient into the prone position results in immediate transfer of lung density from the dorsal to ventral regions. The dorsal lung mass is anatomically greater, hence improved ventilation and enlistment of the dorsal airspaces exceeds the loss of the ventral sections [11].
Ultimately, prone-induced improvements in lung homogeneity promotes gas exchange [14], hemodynamics [15] and, ostensibly, mitigates stress-raisers as described above. This multitude of salutary physiological effects may explain observed clinical benefits of both PEEP and prone positioning in the most severe forms of ARDS [16, 17].
Best,
References
Gattinoni, L. and M. Quintel, How ARDS should be treated. Critical Care, 2016. 20(1): p. 1.
Gattinoni, L. and A. Pesenti, The concept of “baby lung”. Intensive Care Med, 2005. 31(6): p. 776-784.
Protti, A., et al., Lung stress and strain during mechanical ventilation: any safe threshold? Am J Respir Crit Care Med, 2011. 183(10): p. 1354-1362.
Gattinoni, L., et al., Relationships between lung computed tomographic density, gas exchange, and PEEP in acute respiratory failure. Anesthesiology, 1988. 69(6): p. 824-832.
Mead, J., T. Takishima, and D. Leith, Stress distribution in lungs: a model of pulmonary elasticity. J Appl Physiol, 1970. 28(5): p. 596-608.
Cressoni, M., et al., Lung inhomogeneities and time course of ventilator-induced mechanical injuries. The Journal of the American Society of Anesthesiologists, 2015. 123(3): p. 618-627.
JHaitsma, J. and B. Lachmann, Lung protective ventilation in ARDS: the open lung maneuver. Minerva Anestesiol, 2006. 72(3): p. 117.
Cressoni, M., et al., Lung inhomogeneity in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med, 2014. 189(2): p. 149-158.
Caironi, P., et al., Lung opening and closing during ventilation of acute respiratory distress syndrome. Am J Respir Crit Care Med, 2010. 181(6): p. 578-586.
Cressoni, M., et al., Compressive Forces and Computed Tomography–derived Positive End-expiratory Pressure in Acute Respiratory Distress Syndrome. The Journal of the American Society of Anesthesiologists, 2014. 121(3): p. 572-581.
Gattinoni, L., et al., Prone position in acute respiratory distress syndrome. Rationale, indications, and limits. Am J Respir Crit Care Med, 2013. 188(11): p. 1286-1293.
Henderson, A.C., et al., The gravitational distribution of ventilation-perfusion ratio is more uniform in prone than supine posture in the normal human lung. J Appl Physiol, 2013. 115(3): p. 313-324.
Bone, R.C., The ARDS lung: new insights from computed tomography. JAMA, 1993. 269(16): p. 2134-2135.
Chatte, G., et al., Prone position in mechanically ventilated patients with severe acute respiratory failure. Am J Respir Crit Care Med, 1997. 155(2): p. 473-478.
Vieillard-Baron, A., et al., Prone positioning unloads the right ventricle in severe ARDS. CHEST Journal, 2007. 132(5): p. 1440-1446.
Sud, S., et al., Effect of prone positioning during mechanical ventilation on mortality among patients with acute respiratory distress syndrome: a systematic review and meta-analysis. Canadian Medical Association Journal, 2014. 186(10): p. E381-E390.
Goligher, E.C., et al., Oxygenation response to positive end-expiratory pressure predicts mortality in acute respiratory distress syndrome. A secondary analysis of the LOVS and ExPress trials. Am J Respir Crit Care Med, 2014. 190(1): p. 70-76.