

ICU Physiology in 1000 Words: On Venous Capacitance and the U.S. Election

Jon-Emile S. Kenny MD [@heart_lung]
Administering norepinephrine during sepsis resuscitation has a myriad of hemodynamic effects [1]. Importantly, the predominant mechanism probably varies around multiple patient, intervention and time-dependent elements. Most commonly, perhaps, norepinephrine is provided to raise ‘mean arterial pressure’ – an effect driven by its alpha-agonist stimulation of pre-capillary arterioles. While this plays a role, norepinephrine also mediates the venous side of things – phenomena also acting as U.S. citizens contemplate their collective political future.
Vascular Capacitance and Compliance
Capacitance refers to a given vascular pressure at a specific volume [2-4]. It is slightly different from compliance which relates a change in volume to change in pressure. As a rough analogy think of capacitance as the shape of a container into which volume is placed. A petri dish and a graduated cylinder might hold the same volume, but the hydrostatic pressure [i.e. fluid height] generated in the cylinder is larger – it has diminished capacitance. The compliance of the containers might be described by the material from which they are made. A rubber cylinder has a greater compliance than a steel petri dish. Thus, compliance and capacitance are related; capacitance describes how much volume is added before an elastic recoil pressure is generated while compliance describes change in pressure per volume as the recoil pressure starts to rise.
It has been hypothesized that regulating capacitance rather than compliance is an important evolutionary adaptation [5-7]. If significant blood volume is lost [e.g. hemorrhage, or perhaps early septic shock], then augmenting pressure for a smaller volume [i.e. diminished capacitance] would maintain recoil pressure in the veins. By contrast, altering compliance would be moot if the contained volume is too small to engage elastic recoil [Figure 1].
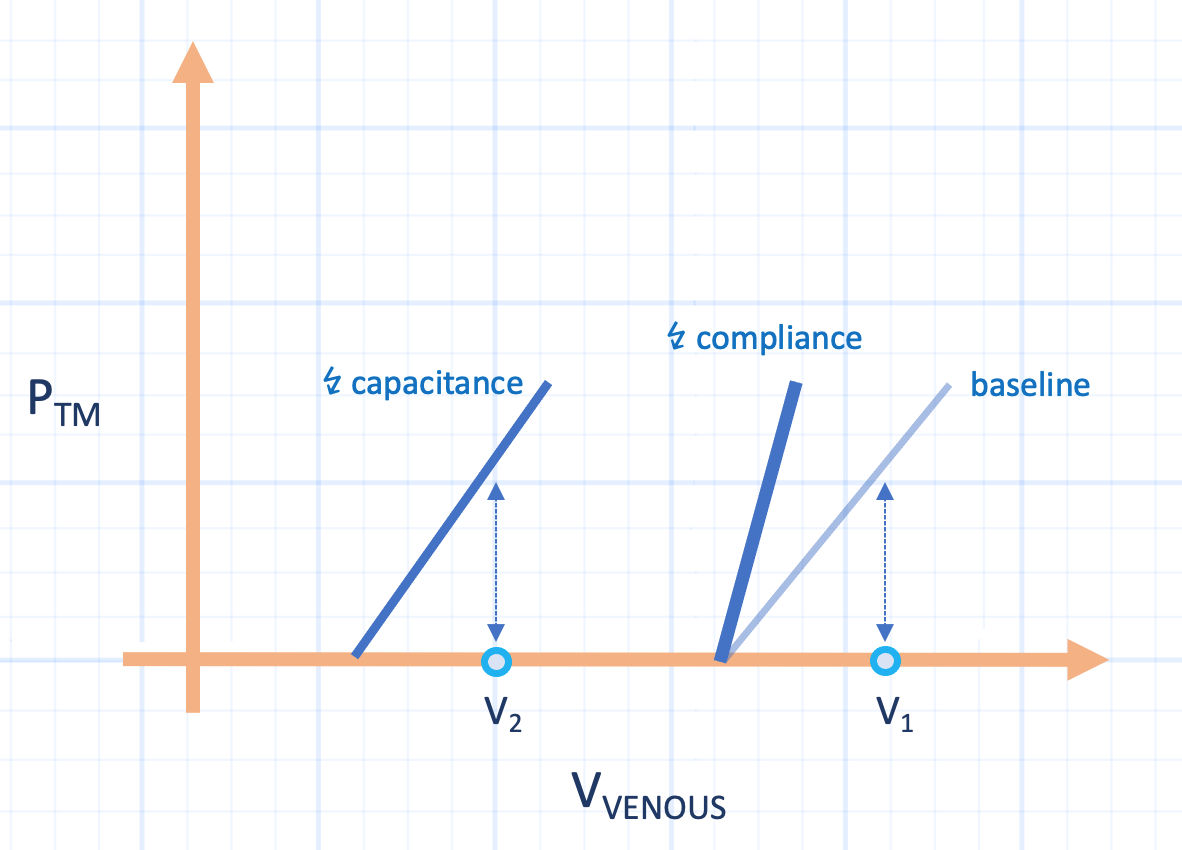
Figure 1: Stylized capacitance diagram. Abscissa is venous volume, ordinate is transmural vein pressure. Baseline characteristics reveal a given pressure for initial volume [V1]. With volume loss [V2], decreasing capacitance maintains the same pressure. Only decreasing the compliance [increased elastance, slope] gives zero transmural pressure at V2.
The effect of norepinephrine on the venous circulation is mostly via capacitance rather than compliance [2, 3]. The latter phenomenon is thought to play a small role in peripheral hemodynamic events. Importantly, for a given blood volume, reflex changes in venous capacitance can effectively ‘add or remove’ approximately 15 – 20 mL/kg of blood volume [2-4]. This has been considered in more detail, previously. While changes in venous capacitance play an important role in resuscitation, they are also likely important in other disease processes such as congestive heart failure – in terms of both disease exacerbation [8] and therapy [9].
Passive and Active Splanchnic Capacitance
The splanchnic circulation plays an important role in the distribution of venous blood volume, and this has been recognized for over a century [2]. A passive change in venous capacitance may follow increased input resistance [e.g. from increased mesenteric arterial resistance]. This may seem paradoxical, but if you imagine an elastic balloon with an input and output orifice and liquid moving into the balloon via the input [e.g. via a hose], the elastic balloon will distend and hold some of the liquid while flow also empties from the output orifice. If you were to then turn off the hose, or slow its flow, the distending pressure of the balloon would shrink – the elastic energy held within the walls would extrude extra volume via the outflow orifice. This is a ‘passive’ decrease in capacitance because it results not from active contraction of the venous walls, but rather passive release of stored elastic energy [2, 3].
By contrast, an active reduction in splanchnic capacitance occurs in response to smooth muscle tension in the venous walls. Adding energy to the venous system by active contraction of veins and venules enhances blood flow to the right heart; if there is reserve in the Frank-Starling mechanism, cardiac output rises. Importantly, it is hard to gauge which mechanism predominates in human hemodynamic unrest; i.e. active or passive. In a canine model, the passive mechanism was noted to contribute roughly two-thirds of the blood volume outflow from the splanchnic circulation and active mechanisms accounted for the remaining one-third [10]. However, in an older, invasive human study of hemorrhage, the splanchnic circulation gave up 40% of its blood volume without a change in flow, suggesting active venoconstriction [11].
While passive mechanisms might predominate in the splanchnic circulation, other venous vascular beds may be different. For example, the hepatic circulation can also redistribute venous blood; yet in this organ, the mechanisms are observed to be more active than passive [4]. Regardless, a key mediator of both active and passive capacitance is alpha receptors on venous vascular smooth muscle and pre-capillary arterioles, respectively.
And the Election?
While there is no direct study of venous capacitance within the current U.S. electorate, one might make some informed inferences. With increasing rates of ‘doom-scrolling’ – the phenomena whereby individuals obsessively and excessively read upsetting news [usually on social media], the venous vasculature might be working silently in the physiological background. Mental stress acts like a catecholamine infusion. Indeed, cognitive load is known to increase heart rate, blood pressure and have variable effects on stroke volume and these responses are associated with systemic release of catecholamines [12]. However, is anything known about mental stress and venous capacitance?
In an older study, a common psychological stress – mental arithmetic – was employed to study the volume-pressure relationship of veins in the forearm [13]. Concurrently, with increased blood pressure and heart rate, radionucleotide plethysmography of the forearm illustrated a ‘left-shift’ in the volume-pressure relationship. At all venous pressures measured, forearm venous volume fell, by about 14%. This is consistent with an ‘active,’ venopressor response and has also been observed in canine limbs following norepinephrine infusion [14]. Importantly, in both the human arithmetic study and other animal studies, the volume-pressure relationship left-shifted without a slope change, indicating diminished capacitance with stable compliance [Figure 1].
Thus, whether a catecholamine infusion is provided to a shocked patient, or consequent to a ‘doom-scrolling’ adrenomedullary reflex-arc [15], venous capacitance is an important element of hemodynamic homeostasis.
Don’t boo – vote,
JE
Dr. Kenny is the cofounder and Chief Medical Officer of Flosonics Medical; he also the creator and author of a free hemodynamic curriculum at heart-lung.org. Download his free textbook here.
References
Foulon P, De Backer D: The hemodynamic effects of norepinephrine: far more than an increase in blood pressure! Annals of Translational Medicine 2018, 6(Suppl 1).
Rothe CF: Physiology of venous return. An unappreciated boost to the heart. Archives of internal medicine 1986, 146(5):977-982.
Rothe CF: Mean circulatory filling pressure: its meaning and measurement. Journal of applied physiology 1993, 74(2):499-509.
Gelman S: Venous function and central venous pressure: a physiologic story. Anesthesiology 2008, 108(4):735-748.
Greenway C, Seaman K, Innes I: Norepinephrine on venous compliance and unstressed volume in cat liver. American Journal of Physiology-Heart and Circulatory Physiology 1985, 248(4):H468-H476.
Greene AS, Shoukas AA: Changes in canine cardiac function and venous return curves by the carotid baroreflex. American Journal of Physiology-Heart and Circulatory Physiology 1986, 251(2):H288-H296.
Shoukas AA, Sagawa K: Control of total systemic vascular capacity by the carotid sinus baroreceptor reflex. Circulation research 1973, 33(1):22-33.
Miller WL: Fluid volume overload and congestion in heart failure: time to reconsider pathophysiology and how volume is assessed. Circulation: Heart Failure 2016, 9(8):e002922.
Tyberg JV: How changes in venous capacitance modulate cardiac output. Pflügers Archiv 2002, 445(1):10-17.
Brooksby GA, Donald DE: Release of blood from the splanchnic circulation in dogs. Circulation research 1972, 31(1):105-118.
Price HL, Deutsch S, Marshall BE et al: Hemodynamic and metabolic effects of hemorrhage in man, with particular reference to the splanchnic circulation. Circulation research 1966, 18(5):469-474.
Hammadah M, Alkhoder A, Al Mheid I et al: Hemodynamic, catecholamine, vasomotor and vascular responses: determinants of myocardial ischemia during mental stress. International journal of cardiology 2017, 243:47-53.
Robinson VJ, Manyari D, Tyberg J et al: Volume-pressure analysis of reflex changes in forearm venous function. A method by mental arithmetic stress and radionuclide plethysmography. Circulation 1989, 80(1):99-105.
Drees JA, Rothe CF: Reflex venoconstriction and capacity vessel pressure-volume relationships in dogs. Circulation research 1974, 34(3):360-373.
Hjemdahl P, Freyschuss U, Juhlin-Dannfelt A et al: Differentiated sympathetic activation during mental stress evoked by the Stroop test. Acta physiologica Scandinavica Supplementum 1984, 527:25-29.