

ICU Physiology in 1000 Words: The Right Atrial Pressure Does Not Determine Cardiac Output – Part 2

Jon-Emile S. Kenny MD [@heart_lung]
In part 1, right atrial pressure [Pra] and cardiac output/venous return [CO/VR] were considered as two hemodynamic measures bound at the operating point [OP] of the circulatory system. Within the sphere of macrohemodynamics, the OP is the true dependent variable – meaning that Pra and CO do not affect each other [1, 2]. The OP, in turn, is governed by the mean systemic filling pressure [Pmsf], pericardial pressure [Ppc], cardiac resistance [i.e., Rcardiac or lumped cardiac function] and the resistance to venous return [Rvr].
Thus, the Pra does not cause the CO and vice versa. In part 1, the concept of association [rather than causation] between Pra and CO was raised. In this second part, we will see that Pra and CO do not associate either! To make this explicit, 2 clinical thought experiments are presented followed by a unifying and practical framework that may be deployed at the bedside.
A tale of two associations
In the first thought experiment, let us consider what happens during passive mechanical ventilation when a series of increasingly-strong inspiratory holds are performed. Importantly, with each inspiratory hold, the Pra and CO are measured; that is, the OP is defined for each hold. To simplify this thought experiment, we have to assume that during these maneuvers the Pmsf, Rvr and Rcardiac remain constant. What would this look like on a Pra – CO graphic [Figure 1A]?
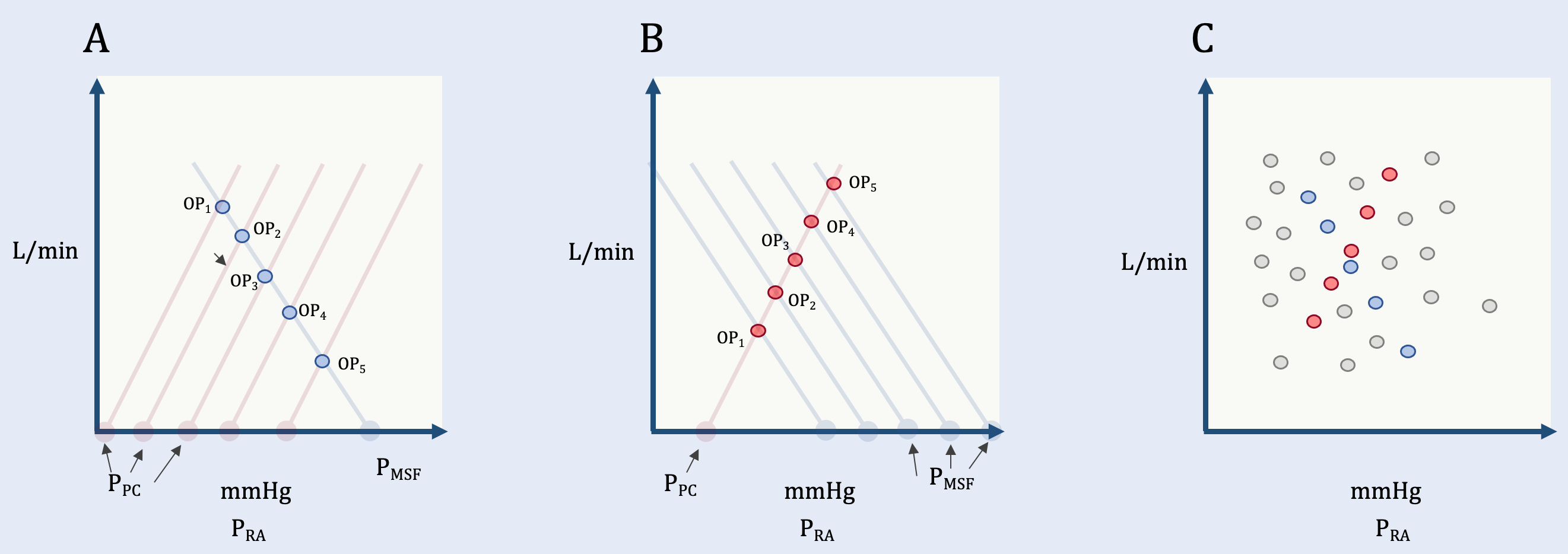
Figure 1: Thought experiments and the simplified geometrical model. The y-axis is CO/VR in litres/min while the x-axis is right atrial pressure in millimetres of mercury. Pra is right atrial pressure, Ppc is pericardial pressure, Pmsf is mean systemic filling pressure. OP is operating point. See text for details. A.] shows inspiratory holds with inverse, linear relationship between Pra and CO/VR; only Ppc is varied here. B.] shows blood administration with a direct linear relationship between Pra and CO/VR; only Pmsf is varied here. C.] Shows what happens when Ppc, Pmsf, Rcardiac and Rvr all vary [grey operating points].
With increasing inspiratory pressure, the Pra rises and CO falls, plotting them reveals a strong, inverse, linear association. Based on the simplified geometrical model, we see the fallacy in concluding that rising Pra causes the fall in CO. Rather, the lurking variable is Ppc. Increased pleural pressure from the ventilator raises Ppc which causes both the Pra to rise and CO to fall. This gives the appearance of causation, but it is an association.
In the second thought experiment, let us consider a patient with significant blood volume loss that is replenished with a series of blood transfusions. Again, to simplify this thought experiment, we assume that Ppc, Rvr and Rcardiac are constant [Figure 1B]. Here, we see that Pra and CO again have a strong association, however, this time it is direct. Based on the simplified geometrical model, we see the fallacy in concluding that rising Pra causes the rise in CO. Rather, the lurking variable is Pmsf. Increased elastic recoil pressure from the peripheral vessels raises Pmsf which causes both the Pra and CO to rise. Again, this gives the appearance of causation, but it is an association.
What happens, if we combine these two thought experiments on to a single Pra – CO graph but also include all of the possible Pra-CO combinations generated by all possible Rvr and Rcardiac slopes? Within the realm of physiologically-possible Pra and CO values, we see that there are an infinite number of operating points! Thus, if a large-enough sample size comprising all possible pathophysiologies was sampled, Pra and CO would have no association [Figure 1C].
Operating point guided resuscitation
How do we make sense of this? The trick, I believe, lies in ‘operating point guided resuscitation’ [OPGR]. What does this mean? For any given hemodynamic state, measure or estimate the Pra and CO [or stroke volume, SV] simultaneously and repeatedly after each intervention. Put another way, because the OP is comprised of both Pra and CO/SV, both values are quantified or qualified at each step of resuscitation. Looking at only venous measures is a one-dimensional approach to resuscitation. In a forthcoming position piece, we argue for a two-dimensional approach by adapting the venerable Diamond and Forrester two-by-two factorial classification [3]. Though this paradigm was initially described in patients following acute myocardial infarction [4], it is easily applied to all states of hemodynamic unrest. How does it work?
First, dichotomize the Pra into ‘low’ versus ‘high.’ This could be done with the Venous Excess Ultrasound Score [VExUS] [5, 6]. A value of zero or 1 is considered ‘low’ while 2 or 3 ‘high.’ Other measures could be used. For instance, an inspiratory IVC collapse of more than 50% classifies patients with a right atrial pressure of less than 10 mmHg [7]. Importantly, however, OPGR doesn’t stop here.
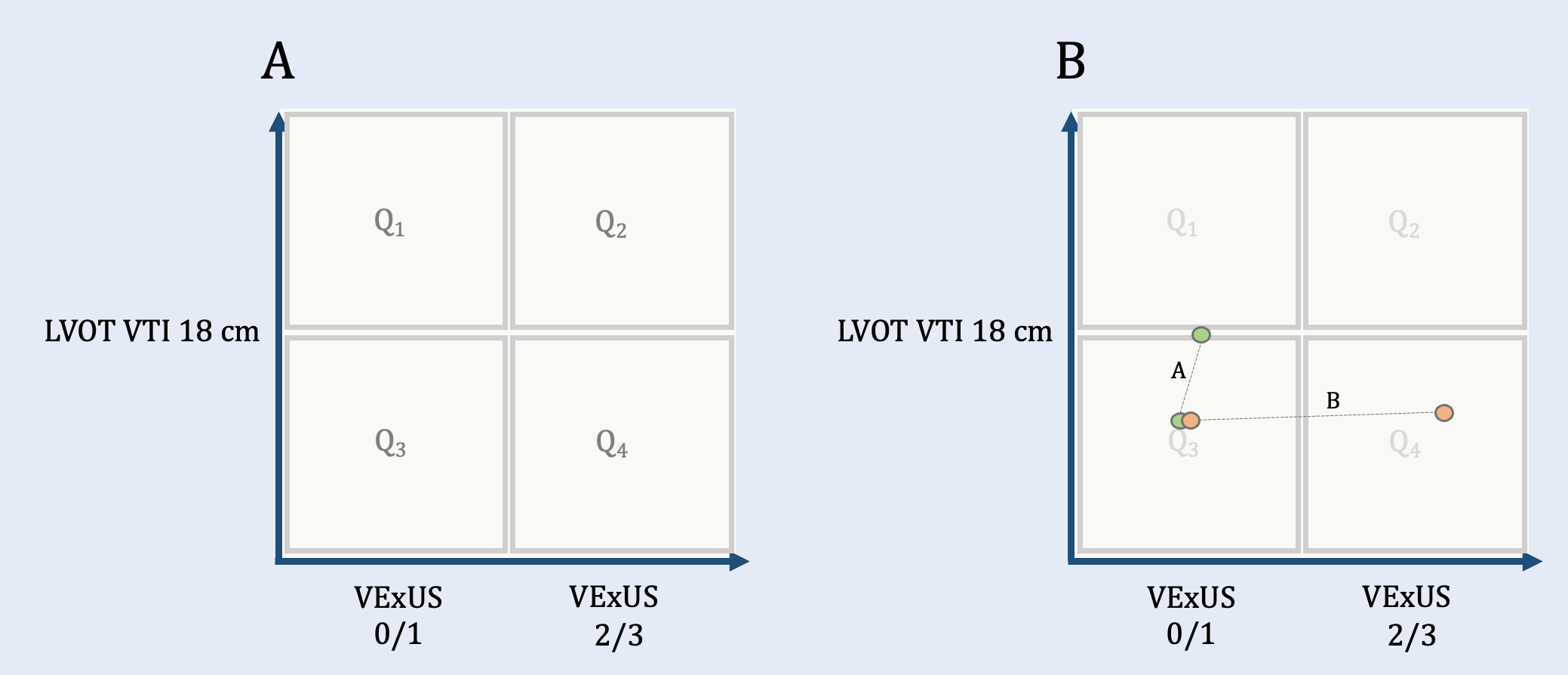
Second, dichotomize SV into ‘normal/high’ or low. This can be made, approximately, by a left ventricular outflow tract velocity time integral measurement [LVOT VTI]. A value of 18 cm or above is considered normal or high while below 18 cm is low [8]. With these thresholds, a two-by-two factorial is created as follows:
Quadrant 1 is ‘normal’ and defined by a VExUS of 0 or 1 and an LVOT VTI of at least 18 cm. Quadrant 2 is ‘warm and congested’ defined by a VExUS of 2 or 3 and an LVOT VTI of at least 18 cm. Quadrant 3 is ‘cold with low filling pressure’ defined by a VExUS of 0 or 1 and an LVOT below 18 cm. Quadrant 4, therefore, is ‘cold and congested’ and consists of a VExUS of 2 or 3 and an LVOT less than 18 cm. How does this work at the bedside?
Clinical examples
Imagine two equally hypotensive patients with prolonged capillary refill time. Both have a hyperdynamic left ventricle, VExUS zero and an LVOT VTI of 10 cm; they are both in Quadrant 3 [Figure 2B], per above. Based on the Diamond and Forrester classification these patients are often called ‘cold and dry’ though we know that there is no relationship between filling pressure and volume status [9]!
As you are not inclined to perform a passive leg raise to test for preload responsiveness, you give both 1 litre of lactated ringers and reassess 30 minutes later. Patient A remains VExUS zero, but her LVOT VTI increased to 17 cm, up towards Quadrant 1. On the other hand, patient B is now VExUS 3 with an LVOT VTI of 12 cm [Figure 2B], out to Quadrant 4. We see that both patients are mathematically ‘preload responsive’, but the change in OP for the two patients reveals two very different cardiac functions! If both remain hypotensive, patient A might respond to additional preload or perhaps, a vasoconstrictor. Patient B on the other hand deserves full echocardiography with emphasis on correcting and treating underlying pump dysfunction [3].
To conclude, Pra and CO do not cause one another, nor do they mathematically associate. Like the Venetian Marionette described some years ago, this may come across as chaos. However, the venerable Diamond - Forrester classification is the stage upon which the OP moves. With patience and practice OPGR directs which circulatory strings to pull and the erstwhile, haphazard hemodynamic gyrations give way to confident and directed movements.
Best,
JE
Dr. Kenny is the cofounder and Chief Medical Officer of Flosonics Medical; he also the creator and author of a free hemodynamic curriculum at heart-lung.org. Download his free textbook here and check out the remainder of this series.
References
1. Kenny JS: A framework for heart-lung interaction and its application to prone position in the acute respiratory distress syndrome. Front Physiol 2023, 14:1230654.
2. Guyton AC: Determination of cardiac output by equating venous return curves with cardiac response curves. Physiol Rev 1955, 35(1):123-129.
3. Kenny J-E, Prager R, Rola P, Haycock K, Basmaji J, Hernández G: Unifying Fluid Responsiveness and Tolerance with Physiology: a dynamic interpretation of the Diamond-Forrester classification Crit Care Explor 2023, (in press).
4. Forrester JS, Diamond G, Chatterjee K, Swan HJ: Medical therapy of acute myocardial infarction by application of hemodynamic subsets (first of two parts). N Engl J Med 1976, 295(24):1356-1362.
5. Longino A, Martin K, Leyba K, Siegel G, Gill E, Douglas IS et al: Correlation between the VExUS score and right atrial pressure: a pilot prospective observational study. Crit Care 2023, 27(1):205.
6. Beaubien-Souligny W, Rola P, Haycock K, Bouchard J, Lamarche Y, Spiegel R et al: Quantifying systemic congestion with Point-Of-Care ultrasound: development of the venous excess ultrasound grading system. The ultrasound journal 2020, 12(1):1-12.
7. Kircher BJ, Himelman RB, Schiller NB: Noninvasive estimation of right atrial pressure from the inspiratory collapse of the inferior vena cava. Am J Cardiol 1990, 66(4):493-496.
8. Mercadal J, Borrat X, Hernández A, Denault A, Beaubien-Souligny W, González-Delgado D et al: A simple algorithm for differential diagnosis in hemodynamic shock based on left ventricle outflow tract velocity-time integral measurement: a case series. Ultrasound J 2022, 14(1):36.
9. Shippy CR, Appel PL, Shoemaker WC: Reliability of clinical monitoring to assess blood volume in critically ill patients. Critical care medicine 1984, 12(2):107-112.