

ICU Physiology in 1000 Words: The Geometry of Ejection Fraction

Jon-Emile S. Kenny MD [@heart_lung]
The left ventricular ejection fraction [LVEF] is a commonly-sought cardiac measure. With the explosion of bedside ultrasound and automated methods to capture LVEF, the ejection fraction will grow in clinical prominence and affect decisions for the acutely-ill. Asked the meaning of the LVEF, many clinicians might describe it as a ‘measure of cardiac function’ – but this is a nebulous answer. Does ‘cardiac function’ mean the contractile or inotropic state? Or does it mean cardiac preload reserve? That is, does the LVEF speak specifically to the slope of the Frank-Starling, or Sarnoff, cardiac function curve ?
This brief articulation of the LVEF will begin with a geometric proof that the LVEF is actually a measure of ventriculoarterial coupling [VAC] [1-3]; this carries two clinical implications. First, the LVEF is not wholly a measure of inotropic state and second, the LVEF ignores the left ventricular lusitropic state. Accordingly, a normal LVEF may be witnessed in a patient with depressed contractility and/or in a patient with cardiac fluid intolerance, respectively.
Ventriculoarterial Coupling
Coupling of the LV to the arterial tree has been considered previously. This model originates from the ground-breaking work of Sagawa, Sunagawa and their colleagues [4]. VAC considers the ratio of the arterial elastance [Ea] to the end-systolic elastance [Ees] as a measure of energetic coupling between the LV and arteries. Normal VAC values range between roughly 0.5 and 1.0 [1]. Critically, the LVEF is described entirely by the Ees and Ea. But how?
End-systolic elastance [Ees]
Recall that the LV pressure-volume loop is a model of ‘time-varying elastance’ – from the relatively low elastance at end-diastole [i.e., the end-diastolic pressure volume relationship, EDPVR], to the high elastance at end-systole [i.e., the end-systolic pressure volume relationship, ESPVR] [1-6]. Notably, the ESPVR is a, largely, load-insensitive measure of inotropic [or contractile] state. A great or diminished slope of the ESPVR speaks to high or low contractility, respectively. The ESPVR is also known as end-systolic elastance [Ees] or maximal elastance [Emax]; Ees is typically used when describing how the LV couples to the arterial tree. As seen in Figure 1, the slope of the Ees is calculated as the ratio of end-systolic pressure [Pes] to end-systolic volume [ESV].
Arterial Elastance
The arterial load faced by the LV is described by the ‘three-element windkessel model,’ which is a challenging measure of afterload to obtain clinically [1]. Thus, the arterial elastance [Ea] is used as a ‘lumped’ surrogate of the afterload. The Ea is insensitive to preload and contractility and is in the same units as Ees because it measures a change in pressure [mmHg] for a change in volume [mL]. The slope of Ea is measured as the end-systolic pressure [Pes] relative to the stroke volume [SV]. The ratio of the Ea to Ees defines VAC, as above.
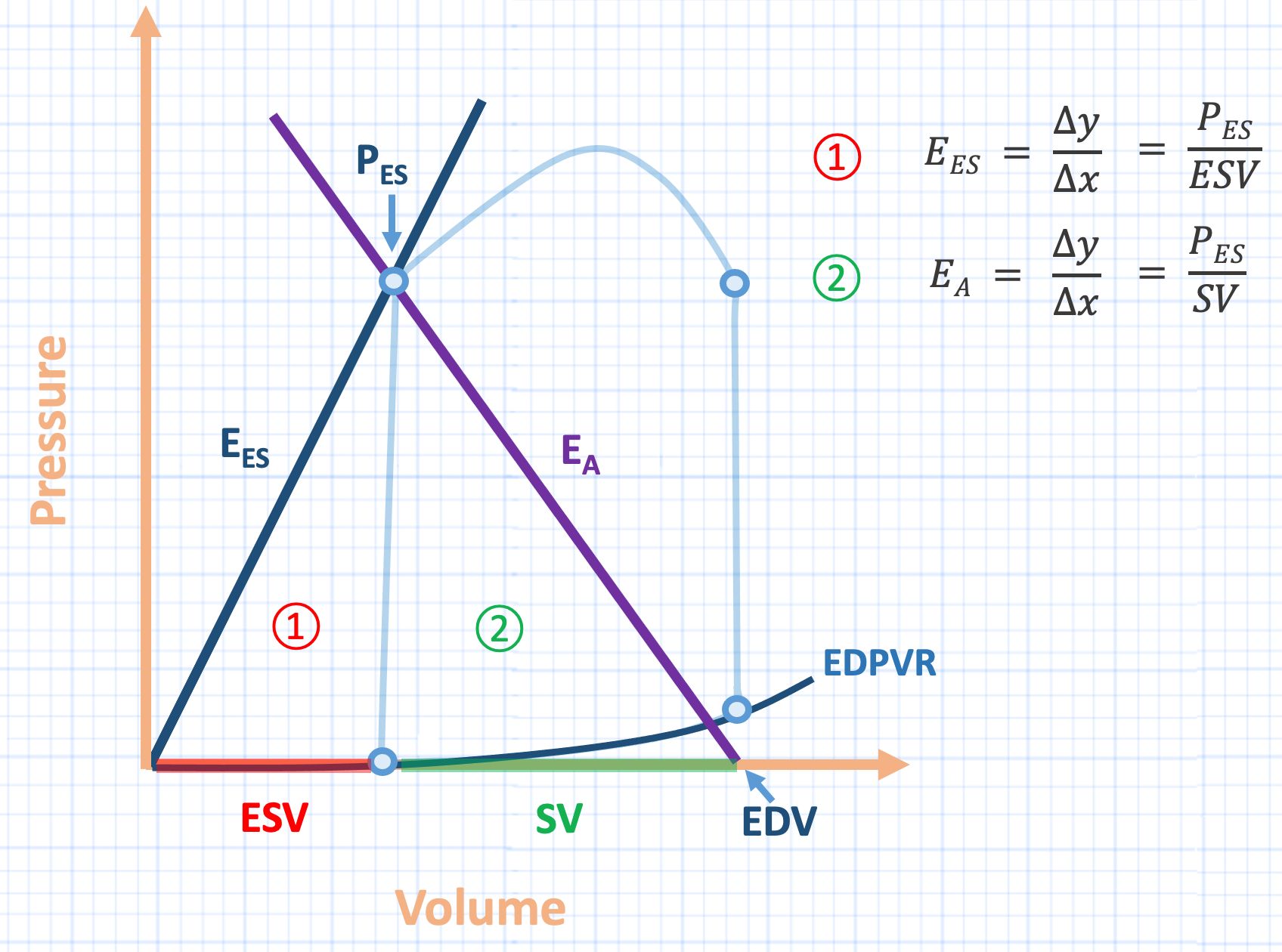
Figure 1: Illustration of ventricular pressure-volume loop [light blue], with superimposed arterial elastance [Ea, purple line]. Pes is end-systolic pressure, Ees is end-systolic elastance, ESV is end-systolic volume, SV is stroke volume, EDV is end-diastolic volume, EDPVR is end-diastolic pressure-volume relationship. Note the two right triangles formed by the slopes of Ees and Ea. Note also that this analysis assumes a left ventricular unstressed volume [Vo] of zero, or the Ees passing through the origin. When Vo is >> than zero, this approach is not valid. The slope of the hypotenuse of triangle 1 is the Ees defined as Pes over ESV. The slope of the hypotenuse of triangle 2 is the Ea defined as the Pes over SV. Ea is considered a positive slope with respect to the arterial tree during systole [i.e., rising pressure with rising volume].
Conjoined Triangles of Left Ventricular Success
Careful inspection of the LV pressure-volume loop with superimposed Ea reveals two, adjacent right triangles, labeled 1.] and 2.] in Figure 1. The base of right triangle 1.] is the end-systolic volume [ESV, red], its vertical cathetus is the end-systolic pressure [Pes] and its hypotenuse is the Ees, as above. The base of right triangle 2.] is the stroke volume [SV, green], its vertical cathetus is also Pes and its hypotenuse is the Ea, as above.
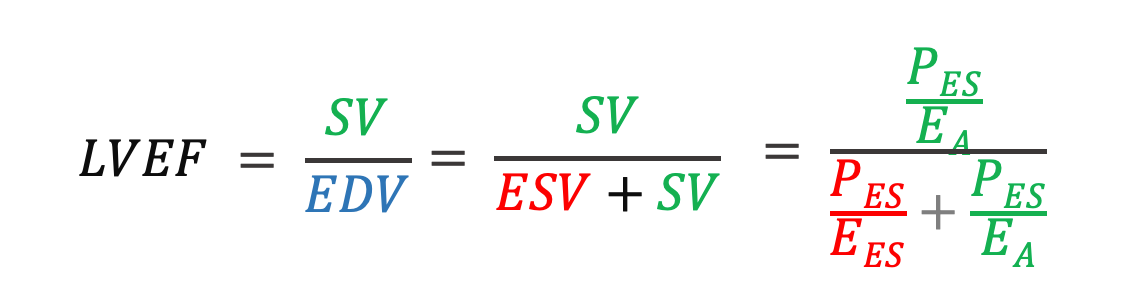
Therefore, by rearrangement, we can express the bases of these triangles as follows:

Note also from Figure 1 that ESV + SV is the end-diastolic volume [EDV]. Accordingly, the equation for LVEF may be expressed as:
With some tidying up to spark joy:
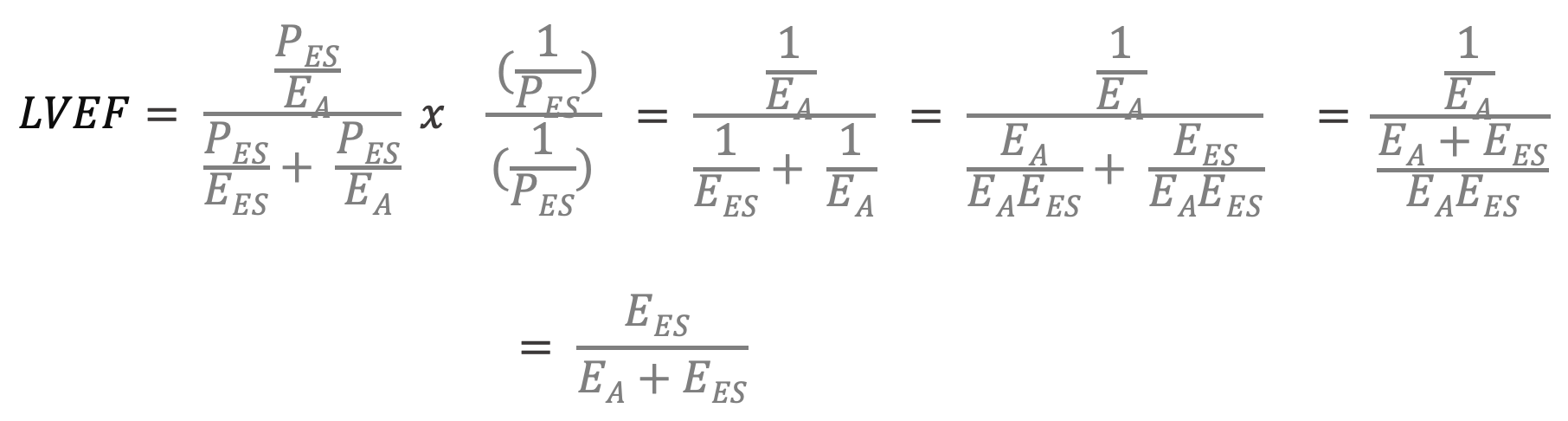
Therefore, LVEF may be equally described as the ratio of Ees [e.g., inotropic state] to the Ees plus Ea [i.e., afterload], that is, ventriculoarterial coupling [3]!
Clinical Implications
First, because the LVEF is described wholly by the relationship between the Ea and Ees, the Ees may be severely depressed, [e.g., septic cardiomyopathy], but if the afterload, Ea is reduced in proportion [e.g., septic vasodilation], then the observed LVEF will be normal – hiding the reduced inotropic state. This would be a similar physiology to a patient with severe, ischemic cardiomyopathy receiving vasodilators. Mathematically, a patient with a supranormal Ees and a Pes of 180 mmHg will have the same LVEF as someone with an Ees reduced by more than 60% and a Pes of 30 mmHg [3]. Thus, seeing a normal LVEF does not necessarily mean that contractile state is normal [Figure 2]! Analogously, a pH of 7.4 does not necessarily mean that there is no acid-base abnormality; there be compensatory mechanisms at play.
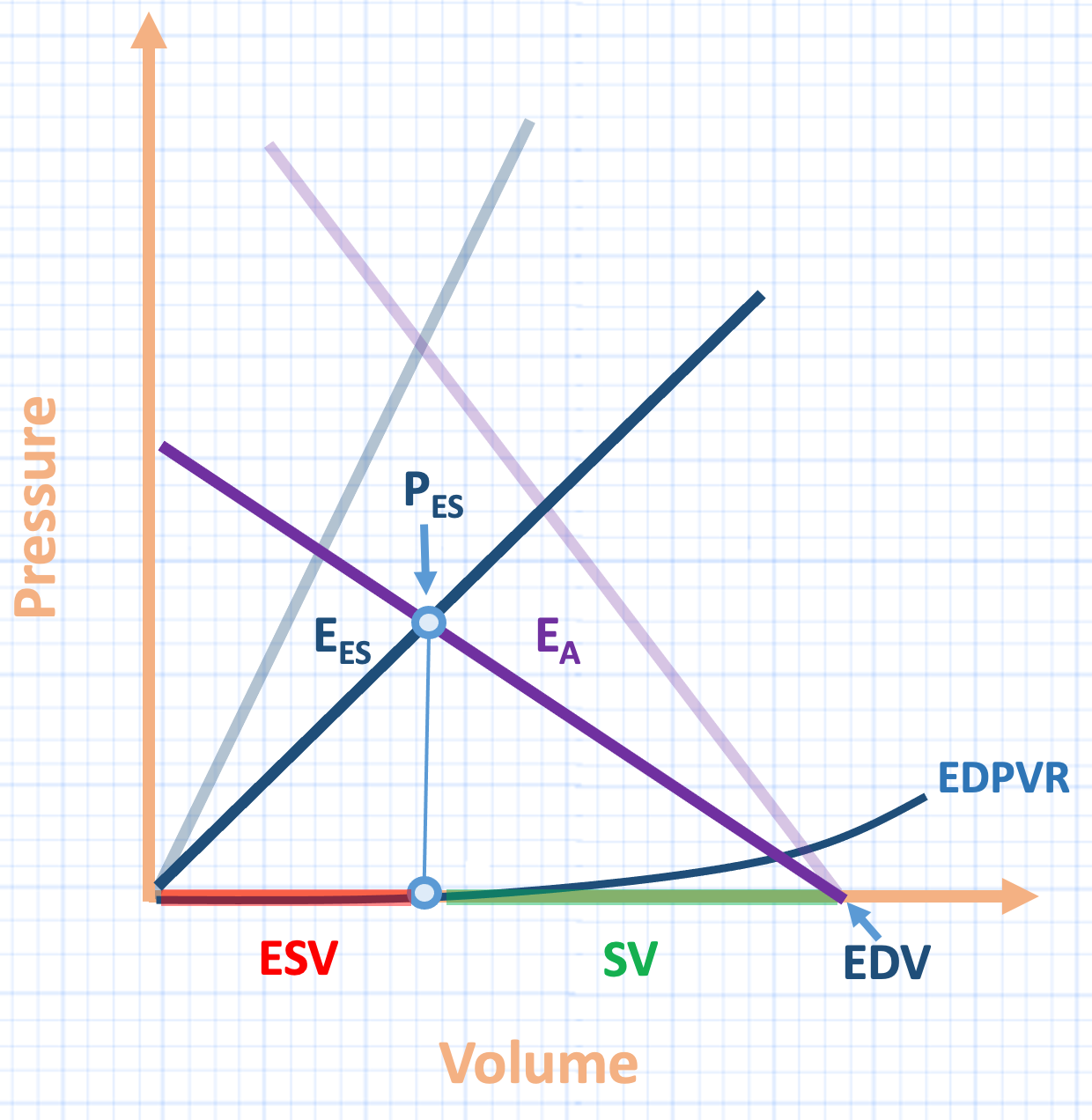
Figure 2: Hypothetical reduction in inotropic state [Ees], with proportional reduction in arterial elastance [Ea]. Note that despite significantly reduced inotropy, the LVEF is unchanged.
Second, because the LVEF is described wholly by the relationship between the Ea and Ees, the ejection fraction is blind to abnormalities in LV lusitropy, or LV relaxation. Consequently, in a hypotensive septic patient with significantly-impaired LV relaxation, it is tempting to think that there is preload reserve and that stroke volume will rise with additional intravenous fluid when the observed LVEF is normal. However, giving the LV additional volume might only enhance LV filling pressure and not SV. This is because when there is impaired LV lusitropy, the left ventricular end-diastolic pressure volume relationship is shifted up and leftwards on the pressure-volume loop [7] such that the ventricle is resistant to increasing its end-diastolic volume [8-11]. Accordingly, additional preload – whether by intravenous fluid or decreased venous capacitance – augments only left ventricular end-diastolic pressure. This might partly explain why a normal ejection fraction does not adequately inform the clinician about cardiac fluid tolerance. Perhaps measures of venous Doppler will offer additional insights and alert the clinician to the very real possibility of a normal ejection with aberrant cardiac function.
Best,
JE
Dr. Kenny is the cofounder and Chief Medical Officer of Flosonics Medical; he is also the creator and author of a free hemodynamic curriculum at heart-lung.org. Download his free textbook here.
References
García MIM, Santos A: Understanding ventriculo-arterial coupling. Annals of Translational Medicine 2020, 8(12).
Guarracino F, Baldassarri R, Pinsky MR: Ventriculo-arterial decoupling in acutely altered hemodynamic states. Critical Care 2013, 17(2):213.
Robotham JL, Takata M, Berman M, Harasawa Y: Ejection fraction revisited. Anesthesiology (Philadelphia) 1991, 74(1):172-183.
Sunagawa K, Maughan WL, Burkhoff D, Sagawa K: Left ventricular interaction with arterial load studied in isolated canine ventricle. American Journal of Physiology-Heart and Circulatory Physiology 1983, 245(5):H773-H780.
Guarracino F, Ferro B, Morelli A, Bertini P, Baldassarri R, Pinsky MR: Ventriculoarterial decoupling in human septic shock. Critical Care 2014, 18(2):R80.
Walley KR: Left ventricular function: time-varying elastance and left ventricular aortic coupling. Critical care 2016, 20(1):270.
Aurigemma GP, Gaasch WH: Diastolic heart failure. New England Journal of Medicine 2004, 351(11):1097-1105.
Landesberg G, Gilon D, Meroz Y, Georgieva M, Levin PD, Goodman S et al: Diastolic dysfunction and mortality in severe sepsis and septic shock. European heart journal 2012, 33(7):895-903.
Marik P, Bellomo R: A rational approach to fluid therapy in sepsis. BJA: British Journal of Anaesthesia 2016, 116(3):339-349.
Ognibene FP, Parker MM, Natanson C, Shelhamer JH, Parrillo JE: Depressed left ventricular performance: response to volume infusion in patients with sepsis and septic shock. Chest 1988, 93(5):903-910.
Fujimoto N, Borlaug BA, Lewis GD, Hastings JL, Shafer KM, Bhella PS et al: Hemodynamic responses to rapid saline loading: the impact of age, sex, and heart failure. Circulation 2013, 127(1):55-62.
This is really well written. Congrats.