

ICU Physiology in 1000 Words: Venous Doppler & Veno-Cardiac Coupling – Part 2

Jon-Emile S. Kenny MD [@heart_lung]
In part 1, the basics of ventriculo-arterial coupling [VAC] were described and related to the Guyton Diagram. In this second part, the notion of cardiac performance [Eh] is explored in relation to venous Doppler velocimetry. Subsequently, I hypothesize that ‘veno-cardiac uncoupling’ – a concept analogous to VAC – is a symptom of poor cardiac performance [Eh]. Lastly, I postulate that abnormal venous Doppler velocimetry indicates ‘veno-cardiac un-coupling’; that is, the aberrant transmission of mechanical power from the venous vasculature to the heart and arterial tree.
Cardiac Performance: Eh
In an imperative read, Parkin and Leaning describe essential tenets of cardiovascular physiology for the intensive care unit [1]. The principles they espouse build upon those initially posed by Guyton [2, 3]. One such premise is cardiac performance [Eh] [4-6]. Essentially, Eh is the slope of the Frank-Starling curve and is described mathematically as the difference between the mean systemic filling pressure [Pmsf] and the right atrial pressure relative to the Pmsf. More concretely, when cardiac performance is excellent, the right atrial pressure falls away from the Pmsf; that is, the difference between them is great. A large difference between these two values raises the value of the numerator of the Eh equation, thus cardiac performance and the slope of the Frank-Starling curve are both considerable [see figure 1A]. By contrast, poor Eh is realized when the right atrial pressure encroaches upon the Pmsf, that is, there is a small difference between them [see figure 1B].
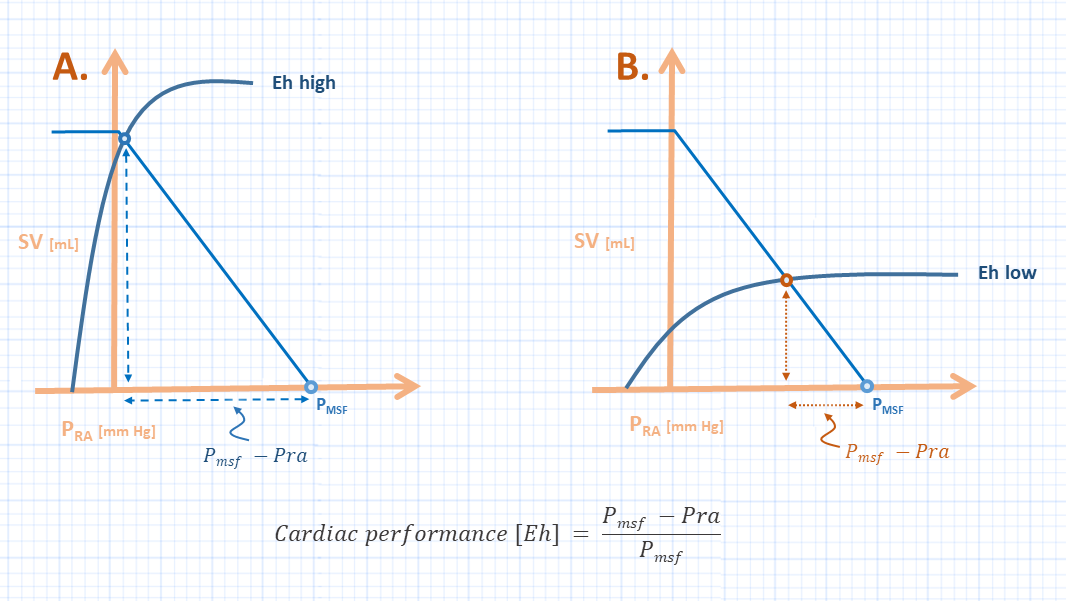
Figure 1: A represents high cardiac performance [Eh] while B represents low cardiac performance. SV is stroke volume, Pra is right atrial pressure, Pmsf is mean systemic filling pressure, the light blue line is venous return while the dark blue curve is the Frank-Starling Curve. Pmsf is determined largely by volume status and venous capacitance; in both patients, Pmsf is the same.
Venous Doppler & Eh
I have previously described the physiology of great vein Doppler velocimetry. A simplified approach to the genesis of the great vein Doppler waveform is to consider it an ‘inverse’ trace of the central venous pressure [CVP or right atrial pressure]. More simply, as CVP falls during a single cardiac cycle, venous velocity rises and vice versa. Consequently, one sees a normal, biphasic systolic and diastolic inflow velocity in conjunction with the x and y descents of the CVP waveform.
It is tempting, therefore, to suppose that as the CVP approaches its upstream pressure [i.e. Pmsf] that venous velocity profiles in distal venous beds become ‘atrialized.’ For example, the portal or intra-renal veins – which typically harbour gentle, undulating velocity patterns – adopt pulsatile velocity profiles that reflect the contour of the CVP. From figures 1A and B, one sees that as Eh worsens, the CVP nears the Pmsf. More clinically, the patient in figure 1A possess a normal intra-renal venous velocity pattern while the patient in 1B exhibits a pulsatile, discontinuous intra-renal venous velocity pattern even though their values of Pmsf are identical!
Mechanical Power and Veno-Cardiac Coupling
Could falling Eh be the physiological explanation for the pulsatile venous velocity patterns seen in heart failure patients [7, 8] and post-cardiac surgery patients [9-12], or are there more universal principles at play?
If we consider the venous return curve with a perfectly performing heart [i.e. Eh = 1.0, or a vertical line], then the area under this [volume-pressure] curve represents the total energy [in joules] of the system [figure 2]. Recall that work over time is power [in Watts] such that if stroke volume becomes cardiac output [i.e. volume over time], then the area under the curve is total power. Thus, an increase in Pmsa increases the total power ‘available’ to the system. From the Guytonian perspective, the heart can only ‘impede’ venous return, should the heart not keep right atrial pressure near maximal venous return – typically atmospheric pressure [3, 13].
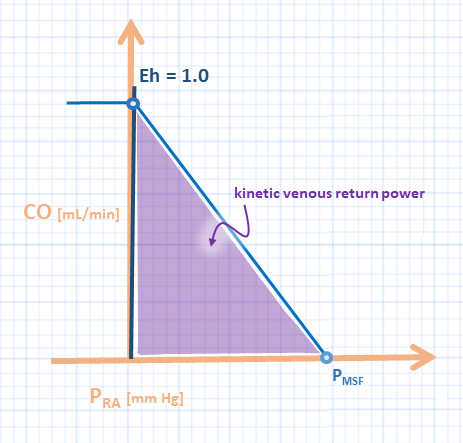
Figure 2: y-axis is cardiac output [HR x stroke volume], while x-axis is Pra or right atrial pressure or central venous pressure. A perfectly performing heart has an Eh of 1.0 and allows total power of venous return to be kinetic. Pmsf is mean systemic filling pressure.
Accordingly, an imperfectly performing heart has its slope shifted down and rightwards [figure 3A]. The area under the cardiac function curve represents passive filling energy. There is an additional power transferred from the venous capacitance beds towards the heart; in effect, this is the conversion of ‘potential work/power’ to ‘kinetic work/power’ from the elastic recoil of the venous vasculature. Thus, when Eh is poor, there is a large portion of cardiac filling power relative to kinetic venous return power [Figure 3A, purple relative to blue shade]; that is, ‘veno-cardiac uncoupling.’ High potential work/power [see part 1] relative to low kinetic venous return power may explain the reflected Doppler velocities seen in the great veins of patients with poor cardiac function and/or high Pmsf relative to cardiac function. Further, 'veno-cardiac uncoupling' suggests a large fraction of ‘potential venous return power’ [red shade] acting upon the veins, venules and organs. Could this be an arbiter of organ dysfunction – analogous to the mechanical power as a mediator of lung injury?
Interestingly, the physiology espoused by Parkin and Leaning [1] has been used to study cardiac power relative to Pmsf as a predictor of volume responsiveness [4, 5]; cardiac power in their studies is different from that described in figure 3 and is defined as cardiac output multiplied by MAP. Nevertheless, cardiac power efficiency levels-off in-step with the plateau of the Frank-Starling curve [5].
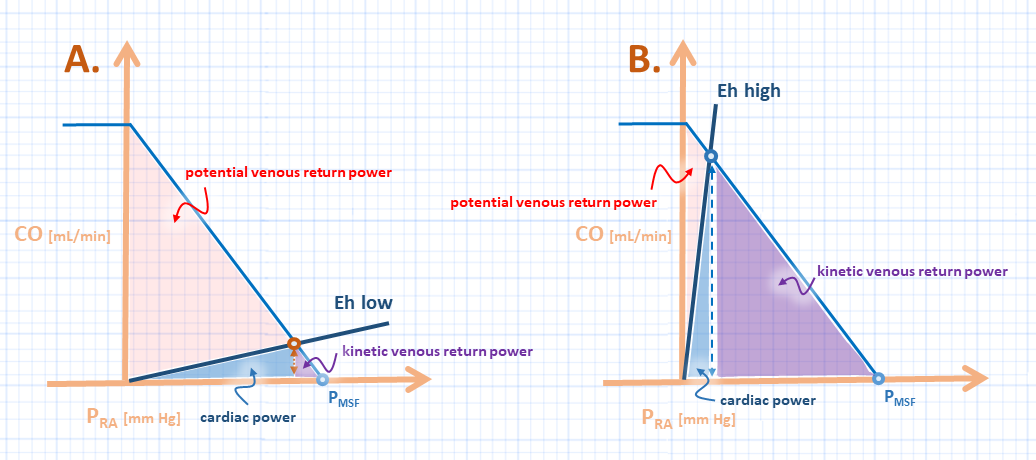
Figure 3: Axes are the same as figure 2. A represents poor cardiac performance and 'veno-cardiac un-coupling' - relate this to ventriculo-arterial uncoupling in figure 1B in part 1. The blue shade is cardiac filling power which, ostensibly, is the area under the EDPVR in figure 1, part 1. It is possible that high potential venous return power [red shade] underpins backwards venous velocity reflections and corresponds to potential work in figure 1 part 1. B represents good cardiac performance or high efficiency - see part 1, figure 1A. Thus there is low cardiac filling power relative to kinetic venous return power [purple shade]. As well, there is low total potential venous return power [red shade]; this corresponds to high cardiac efficiency in part 1.
Venous Doppler: clinical implications
The clinical implications of the above are relatively simple. Reversal of great vein velocity patterns may represent elevated potential venous return power relative to kinetic venous return power; what I term ‘veno-cardiac uncoupling’. It is plausible that imbalance between forward and reverse-focused cardiovascular power mediates organ injury.
Additionally, while hypervolemia favours excessive ‘potential venous return power,’ veno-cardiac coupling is also decided by Eh. This may explain why portal vein pulsatility was recently observed to appear or disappear without large vascular volume shifts [e.g. immediately after induction of anesthesia or upon transfer from the operating room to the ICU] [14]. Further, inhaled vasodilators can abolish venous Doppler velocity pulsations by improving cardiac function [9] without any acute change in volume status.
One potential caveat to the above is that it assumes that venous return and cardiac function are independent. A recent study on intravenous fluids found that volume infusion – that is, increasing Pmsf and venous return – also improved Eh [as described in part 1] [15]. Further, venous Doppler pulsations are modified by factors beyond atrial pressure reflections. For example, portal vein pulsatility is also mediated by arterial pressure reflections through the mesenteric artery [16, 17] as well as body habitus [18].
Accordingly, the results of all diagnostic tests – including Doppler ultrasound – must be interpreted and applied within a specific clinical context!
Celebrating 5 years of this series!
JE
Dr. Kenny is the cofounder and Chief Medical Officer of Flosonics Medical; he is also the creator and author of a free hemodynamic curriculum at heart-lung.org
References
Parkin, W.G. and M.S. Leaning, Therapeutic control of the circulation. Journal of clinical monitoring and computing, 2008. 22(6): p. 391-400.
Parkin, W. and C. Wright, Three dimensional closed loop control of the human circulation. International journal of clinical monitoring and computing, 1991. 8(1): p. 35.
Magder, S., Volume and its relationship to cardiac output and venous return. Critical care, 2016. 20(1): p. 271.
Gupta, K., et al., Applying mean systemic filling pressure to assess the response to fluid boluses in cardiac post-surgical patients. Intensive care medicine, 2015. 41(2): p. 265-272.
Sondergaard, S., J.S. Larsson, and P.W. Möller, The haemodynamic effects of crystalloid and colloid volume resuscitation on primary, derived and efficiency variables in post-CABG patients. Intensive Care Medicine Experimental, 2019. 7(1): p. 13.
Sondergaard, S., G. Parkin, and A. Aneman, Central venous pressure: soon an outcome-associated matter. Current Opinion in Anesthesiology, 2016. 29(2): p. 179-185.
Iida, N., et al., Clinical implications of intrarenal hemodynamic evaluation by Doppler ultrasonography in heart failure. JACC: Heart Failure, 2016. 4(8): p. 674-682.
Tang, W.W. and T. Kitai, Intrarenal venous flow: a window into the congestive kidney failure phenotype of heart failure? JACC: Heart Failure, 2016. 4(8): p. 683-686.
Tremblay, J.-A., et al., Point-of-care ultrasonography to assess portal vein pulsatility and the effect of inhaled milrinone and epoprostenol in severe right ventricular failure: A report of 2 cases. A&A Case Reports, 2017. 9(8): p. 219-223.
Denault, A.Y., et al., Clinical Significance of Portal Hypertension Diagnosed With Bedside Ultrasound After Cardiac Surgery. Anesthesia & Analgesia, 2017. 124(4): p. 1109-1115.
Beaubien-Souligny, W., et al., The Role of Point-of-Care Ultrasound Monitoring in Cardiac Surgical Patients With Acute Kidney Injury. Journal of Cardiothoracic and Vascular Anesthesia, 2018.
Beaubien‐Souligny, W., et al., Alterations in Portal Vein Flow and Intrarenal Venous Flow Are Associated With Acute Kidney Injury After Cardiac Surgery: A Prospective Observational Cohort Study. Journal of the American Heart Association, 2018. 7(19): p. e009961.
Magder, S. and S.M. Scharf, Venous return. Magder, Sheldon, and Steven M. Scharf. "Venous return." LUNG BIOLOGY IN HEALTH AND DISEASE 157 (2001): 93-112.
Eljaiek, R., et al., High postoperative portal venous flow pulsatility indicates right ventricular dysfunction and predicts complications in cardiac surgery patients. British journal of anaesthesia, 2019. 122(2): p. 206-214.
Guarracino, F., P. Bertini, and M.R. Pinsky, Cardiovascular determinants of resuscitation from sepsis and septic shock. Critical Care, 2019. 23(1): p. 118.
Nihei, Y., H. Sasanuma, and Y. Yasuda, Experimental evaluation of portal venous pulsatile flow synchronized with heartbeat intervals. Journal of Medical Ultrasonics, 2011. 38(3): p. 141-149.
Nihei, Y., H. Sasanuma, and Y. Yasuda, Experimental evaluation of portal venous pulsatile flow synchronized with heartbeat intervals: effects of vascular clamping on portal hemodynamics. Journal of Medical Ultrasonics, 2013. 40(1): p. 9-18.
Gallix, B., et al., Flow pulsatility in the portal venous system: a study of Doppler sonography in healthy adults. AJR. American journal of roentgenology, 1997. 169(1): p. 141-144.