

ICU Physiology in 1000 Words: The Mechanical Power & Ventilator-Induced Lung Injury

Jon-Emile S. Kenny MD [@heart_lung]
A few years ago I was intrigued by a new concept in Ventilator-Induced Lung Injury [VILI] – the mechanical power. I employed this paradigm, introduced by Gattinoni’s group, as an opening for the ‘ARDS Trilogy.’ Since then, I have also discussed this ‘ergotrauma’ in the context of helium-oxygen physiology and airway pressure release ventilation [APRV]. With emerging data on mechanical power – and especially a recent report on the interaction between PEEP and mechanical power [1] – a simple exposition on this topic is timely. My goal is to explain the frighteningly complicated mechanical power equation using a clinically-familiar graphic – the ventilator waveform.
Background
Perhaps the leap forward offered by mechanical power is its conceptual parsimony – tying together multiple, incongruent instigators of VILI into a single explanatory variable [2, 3]. And this conceptual frugality is matched by its face-validity in first principles; i.e., power is work over time, work is a force over a distance, necessitating energy transfer, and energy is needed to break stuff – like lung tissue.
From a clinical perspective, tidal volume [i.e. displacement of the lung or its ‘strain’] and trans-pulmonary pressure [i.e. the pressure difference between the airway and the pleural space or ‘stress’] have been undeniably essential mediators of ventilator – or ventilation – induced lung injury; yet, they alone cannot explain other known arbiters of harm. For example, with constant tidal volume and airway pressure, increased respiratory rate is well-known to exacerbate lung injury [4, 5]. Further, with tidal volume, driving pressure and respiratory rate all equal, rapidly delivered volume – i.e. increased flow or strain rate – also promotes lung injury [6, 7]. Importantly, all of these facilitators of VILI are contained – and therefore explained – within the model of the mechanical power applied to the lung [8, 9].
Determinants of Mechanical Power
The equation for mechanical power is shown at the bottom of figure 1; admittedly, this is scary-looking. Yet, read on and you will find that you’ve actually been staring at a graphical representation of this equation thousands of times; let’s break it down.
For simplicity, we will consider inspiration during a ventilator-delivered breath in a passive patient. The classical equation of motion [2, 5, 8, 10, 11] states that at any given moment in time, the pressure in the airway is the summation of two principle components [three if you consider positive end-expiratory pressure - PEEP]. These two components are: 1. the pressure required to overcome airway and tissue resistance and 2. the pressure required to increase the volume of the lung and chest wall. These two components evolve over the duration of a breath and may be thought of analogously to kinetic and potential energy, respectively. In other words, there is pressure dedicated to 1. movement, for example, of gas [i.e. kinetic energy] and 2. the increasing volume of an elastic structure [i.e. potential energy].
These components are often visualized on a pressure-volume curve for a passive, ventilated patient; this is also depicted in figure 1. The kinetic component is the parallelogram shaded in blue – this is often referred to as ‘resistive pressure’ and the area defined by the blue shade is the ‘resistive work.’ By contrast, the potential energy from the tidal volume-related ‘elastic work’ is shaded in red. Finally, when PEEP is applied, there is an additional elastic component of work shaded in pink.
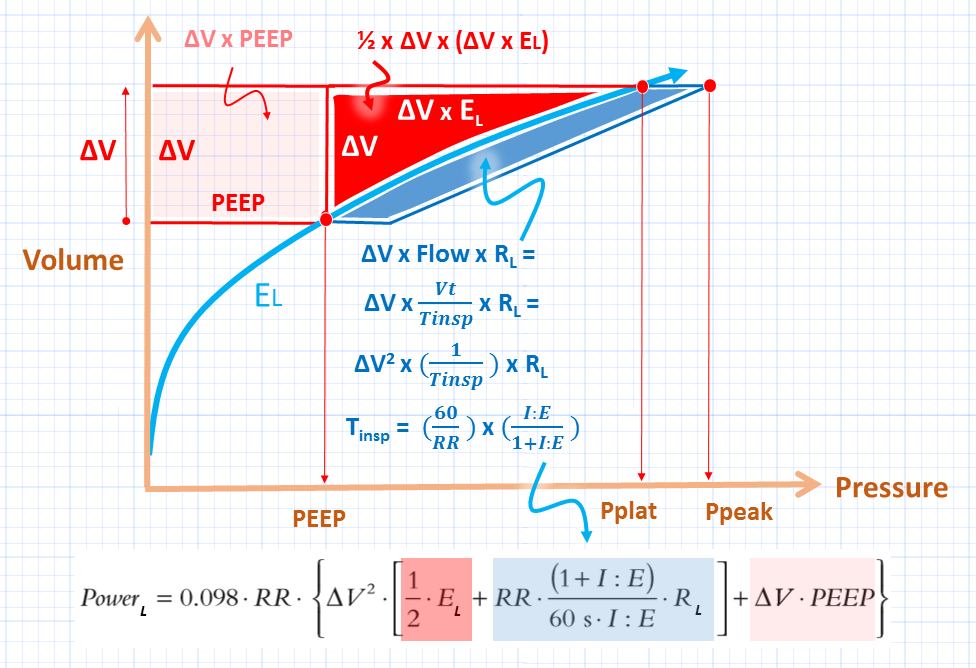
Figure 1: The work for a single breath across the lung and its power over time; volume on the y-axis and pressure on the x-axis. EL is lung elastance, ΔV and Vt are tidal volume, RL is tissue resistance of the lung. Note that this figure assumes that this is the pressure across the lung, as if there were an esophageal manometer. The three components of work per breath are shaded in pink, red and blue [see text]. The derivation of resistive work in blue is given and colour-coded in the power equation at the bottom. 0.098 is the conversion factor from L*cm H2O to Joules. Power is the respiratory rate multiplied by the work of a single breath with its equation [Power L] at the bottom. Pplat is plateau pressure and Ppeak is peak airway pressure. Tinsp is inspiratory time and I:E is the inspiratory-to-expiratory ratio.
Back to the Equation
As the area of each of these three sub-components represent work, they can be summed to obtain the total work for a single inspiration. The areas can be computed by simple geometry because the PEEP-related elastic work [in pink] is a square, the tidal volume-related elastic work [in red] is a triangle and the resistive work, in blue, is approximated by a parallelogram.
The dimensions of each of these shapes can be read from the pressure-volume graph – recall that the area of a square and parallelogram are simply base x height and a triangle is one-half base x height. Note that the ‘height’ of the triangle [its pressure cathetus] can be calculated by multiplying its base [its volume cathetus] by the slope of its hypotenuse. The slope of the hypotenuse is the elastance of the lung [El – elastance is the change in pressure for a change in volume – the inverse of compliance]. The ‘base’ of the parallelogram [in pressure] is the gas flow x tissue resistance [which can be obtained from an end-inspiratory hold] while the height of the parallelogram is tidal volume [ΔV].
Accordingly, when all of these areas are summed, one can see the power equation start to take shape – including the seemingly strange tidal volume [ΔV] squared term. When the work of one breath is multiplied by the respiratory rate, then power over time is given.
Relation to the Pressure Waveform on a Ventilator
As described in this older post on the driving pressure, the pressure-volume curve – so often used in basic respiratory physiology papers – can be transmuted into the pressure-time curve displayed on a ventilator. We can simply move pressure from the x-axis to the y-axis and assume that there is constant flow delivery [i.e. square-wave flow] such that volume and time become linear analogues [i.e. if flow is constant, then the same amount of volume is delivered per unit time]. Now the x-axis becomes time instead of volume. As seen in figure 2, you have undoubtedly already subdivided a breath into its elastic and resistive work components when performing an end-inspiratory hold to differentiate peak from plateau pressures; you are already intimately familiar with mechanical power.
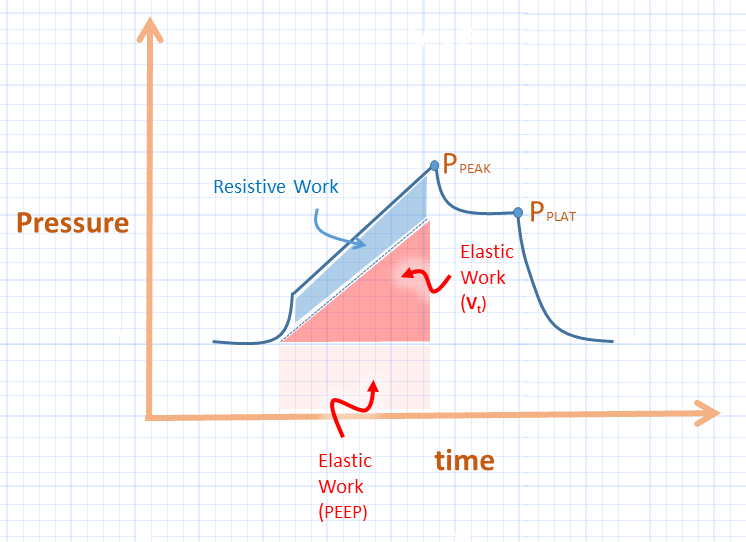
Figure 2: Pressure-time waveform from a ventilator. This is slightly different from figure 1 in that the waveform on the ventilator represents the lung and chest wall in series. To determine the stress across the lung, an esophageal balloon would be required to assess the elastance of the lung. The colours on the ventilator waveform correspond to the areas of work shown for the lung in figure 1. Vt is tidal volume
Controversy
While mechanical power deserves our complete attention, it is not without criticism [12] especially in light of two recent papers on the interaction between tidal volume and power [13] and PEEP and power [1]. While all of power seems important, should we preferentially focus on the ‘driving power’ as coined by Marini [2]? I will explore this shortly.
Please check out other articles in this series,
JE
Dr. Kenny is the cofounder and Chief Medical Officer of Flosonics Medical; he is also the creator and author of a free hemodynamic curriculum at heart-lung.org
References
Collino, F., et al., Positive end-expiratory pressure and mechanical power. Anesthesiology: The Journal of the American Society of Anesthesiologists, 2019. 130(1): p. 119-130.
Marini, J.J. and S. Jaber, Dynamic predictors of VILI risk: beyond the driving pressure, 2016, Springer.
Gattinoni, L., et al., The future of mechanical ventilation: lessons from the present and the past. Critical Care, 2017. 21(1): p. 183.
Marini, J.J., J.R. Hotchkiss, and A.F. Broccard, Bench-to-bedside review: microvascular and airspace linkage in ventilator-induced lung injury. Critical Care, 2003. 7(6): p. 435.
Tonetti, T., et al., Driving pressure and mechanical power: new targets for VILI prevention. Annals of translational medicine, 2017. 5(14).
Protti, A., et al., Lung stress and strain during mechanical ventilation: any difference between statics and dynamics? Crit Care Med, 2013. 41(4): p. 1046-1055.
Protti, A., E. Votta, and L. Gattinoni, Which is the most important strain in the pathogenesis of ventilator-induced lung injury: dynamic or static? Curr Opin Crit Care, 2014. 20(1): p. 33-38.
Gattinoni, L., et al., Ventilator-related causes of lung injury: the mechanical power. Intensive Care Med, 2016. 42(10): p. 1567-1575.
Cressoni, M., et al., Mechanical power and development of ventilator-induced lung injury. Anesthesiology: The Journal of the American Society of Anesthesiologists, 2016. 124(5): p. 1100-1108.
Otis, A.B., W.O. Fenn, and H. Rahn, Mechanics of breathing in man. J Appl Physiol, 1950. 2(11): p. 592-607.
Marini, J.J. and P.S. Crooke, A general mathematical model for respiratory dynamics relevant to the clinical setting. American Review of Respiratory Disease, 1993. 147: p. 14-14.
Huhle, R., et al., Is mechanical power the final word on ventilator-induced lung injury?—no. Annals of translational medicine, 2018. 6(19).
Santos, R.S., et al., Biologic impact of mechanical power at high and low tidal volumes in experimental mild acute respiratory distress syndrome. Anesthesiology: The Journal of the American Society of Anesthesiologists, 2018. 128(6): p. 1193-1206.
Has your opinion changed since the 4dprr paper from Dr Amato ? Maybe focus on Dp and rr rather than whole power ?